Download
1 / 6
60 likes | 74 Views
This study examines the prevalence of gaming disorder among a sample of Mexican college freshmen using DSM-5 criteria. The findings suggest a significant percentage of students exhibiting severe impairment in various life domains. The study also explores the association between gaming disorder and mental health treatment utilization.

E N D
10-10-18 Gaming disorder among a sample of Mexican college freshmen.Guilherme Borges, Ricardo Orozco and Corina BenjetInstituto Nacional de Psiquiatría Ramon de la Fuente Muñiz, Calzada México Xochimilco No. 101, Col. San Lorenzo Huipulco, CP: 14370, CDMX, México.E-mail address: guibor@imp.edu.mx Diagnostic/Screening/Assessment of Internet/Gaming Addiction panel at the upcoming Digital Media and Developing Minds Cold Spring Harbor Laboratory, 7:30-8:15 pm Tuesday, October 16th, 2018.
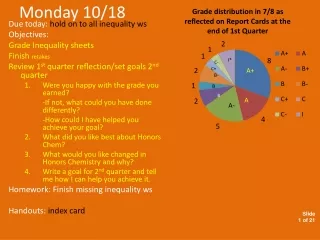
1.Wendy Feng et al., 2017: Internet gaming disorder: Trends in prevalence 1998–2016 Fig. 2. IGD prevalence over time (N =27 studies in natural populations; 23 different scales). The average percentage was 4.7% across all years (range 0.7-15.6%). DSM-5 (2013) 2.JIA YUIN FAM et al., (2018):Prevalence of internet gaming disorder in adolescents: A meta-analysis across three decades Overall: 28 estimates since 1998; 4.6% (range 3.4-6.0%) (IGD strict sense= 1.6%; If sample size>5,000= 2.2%. 3.Mihara and Higuchi, 2017: Cross-sectional and longitudinal epidemiological studies of Internet gaming disorder: A systematic review of the literature. Up to May 2016- 37 cross-sectional (prevalence 0.7%-27.5%) and 13 longitudinal studies. 4.Paulus et al., 2018: Internet gaming disorder in children and adolescents: a systematic review. 41 studies prevalence ranged 0.6%-50%, median 5.5%. Median prevalence for 10 population based studies: 2.0% 5.Petry et al., 2018: Behavioral Addictions as Mental Disorders: To Be or Not To Be?. 9 studies sample size >3,000 respondentes prevalence ranged 0.3%-4.9%.
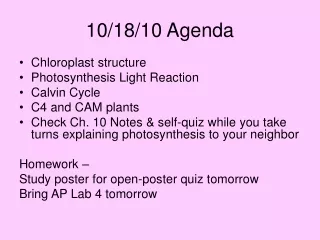
Prevalence DSM-5 IGD byauthor (14 authors; 17 studies)-year (2015-2018) in total population (14 estimatesleft-range 1.16%-10.80%) and amonggamers (8 estimatesright- range 2.90%-13.80%) Random meta-regression Prev= 5.5% (95%CI-3.8-7.3%) Pontes, 2016: 7 scalesfor DSM-5; Almeida, 2018: 11 scalesfor DSM-5 Random meta-regression Prev= 3.5% (95%CI-2.6-4.5%)
METHODS- DSM-5/IGD (total sample 5.6%; gamers 8.9%): males (10.8%)-females (1.8%); age 18-19 (5.1%)- age 20+ (7.3%) • Sample: Incoming first year students in Mexican universities. For this first analyses on gaming, sample consisted of N=3,799 students (63.5% gamers, 53.6% females, 75.1% 18-19 y/o) (and counting). Participants gave consent and were given access through a web-based survey, had to be at least 18 years of age to participate. Item Response Theory (IRT) main results for gamers: unidimensionaly with factors loading between 0.801-0.923. Cronbach's α = 0.8564 – Items from G and SU work well and are mingled together
DSM-5 “leading to clinically significant impairment or distress”; ICD-11 “significant impairment in personal, family, social, educational, occupational or other important areas of functioning. Here, severity of health-related role impairment assessed by using an adapted version of the Sheehan Disability Scale. Four role domains: home management/chores, college-related and other work, close personal relationships, and social life. No interference (0), mild (1–3), moderate (4–6), severe (7–9), and very severe (10) interference. IGD+ were at increase odds of showing severe/very severe: home management/chores (2.1(0.9-4.8)), college-related and other work (3.2*(1.9-5.3)), close personal relationships (1.6(0.9-2.9)), and social life (1.7(0.9-2.9)). In summary total severe/very severe: 2.3*(1.6-3.5) In the total sample(3,779), IGD+(214) were more likely to: lifetime use of any psychological TX (aOR=1.6*(1.1-2.3)); any medical TX (1.9*(1.0-3.7)).
DISCUSSION- Some limitations are apparent • DSM-5 frame has became predominant, but scales abound everywhere. ICD estimates to come next with its own scales and prevalence estimates? • Common approach used with prior addictions (alcohol, tobacco, drugs) framework (Item Response Theory- IRT) is sometimes available. Need to put IRT results all together (unidimensionality; discrimination&difficulty; INVARIANCE-DIF). • Mostly on children and adolescents. Sometimes broad age range and few estimates for adults only. Range of prevalence is not bad by itself (see SUD). • Some with few number of cases. We lack estimates from traditional epidemiological framework for sample representativeness (large community surveys). • Besides the few clinical studies, some studies are on selected samples of respondents in web sites (no response rates)- not good for population prevalence estimates. • Some reports on gamers only (not common definition). Do we need a definition of “gamers”? • Few, if any, external validators in non-clinical samples. Few discussion on impact on service use and/or impairment (DSM and ICD “extra” criterion). • Few (any?) studies in western low-middle income countries.