Download
1 / 103
1.06k likes | 1.17k Views
Aortic Arch Anomalies. Development of Aortic Arch and great vessels. Anatomical Categories. Abnormalities of branching Normal L Aortic Arch & Variants Abnormal L Aortic Arch Abnormalities of arch position 3. R Aortic Arch 4. Cervical Aortic Arch Superpneumarary arches

E N D
Anatomical Categories • Abnormalities of branching • Normal L Aortic Arch & Variants • Abnormal L Aortic Arch • Abnormalities of arch position 3. R Aortic Arch 4. Cervical Aortic Arch • Superpneumarary arches 5. Double Aortic Arch 6. Persistent Fifth AA 7. Interrupted Aortic Arch 8. Anomalous origin of PA branches and other AA anomalies
Clinical Classification • Vascular rings • Non ring vascular compression of trachea, bronchi, oesophagus • Non compressive arch malformation • Duct dependent arch anomalies
Clinical features of vascular rings • Stridor – increase with RTI • Recurrent pneumonia/ bronchitis • Hyperextension of neck (esp. in infants) • Reflex apnoea associated with eating • Swallowing difficulty • Chocking of food
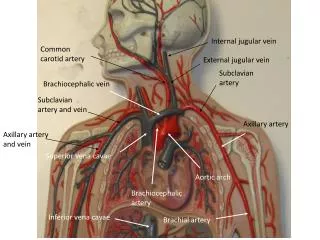
Sidedness of Aortic arch • L & R aortic arch definitions • Refers to which bronchus is crossed by the arch • Normal – • Cross the L main bronchus at T5 • Branching…. general rule – 1st arch vessel contain a carotid a. contralateral to Ao A • Importance of sidedness of Ao arch • BT shunt – on side of In A • Repair of oesophageal atresia – side opp arch
Anatomical Categories • Abnormalities of branching • Normal L Aortic Arch & Variants • Abnormal L Aortic Arch • Abnormalities of arch position 3. R Aortic Arch 4. Cervical Aortic Arch • Superpneumarary arches 5. Double Aortic Arch 6. Persistent Fifth AA 7. Interrupted Aortic Arch 8. Anomalous origin of PA branches and other AA anomalies
1. Normal L Aortic Arch & Variants Variants 1. Common brachiocephalic trunk • Present in 10% of L arches • No consequences
1. Normal L Aortic Arch & Variants Variants 2. Separate origin of L vertebral a. from aortic arch (normal – from L subclavian) • Size 1>2, 3<4 • DD – anomalous R SCA
Anatomical Categories • Abnormalities of branching • Normal L Aortic Arch & Variants • Abnormal L Aortic Arch • Abnormalities of arch position 3. R Aortic Arch 4. Cervical Aortic Arch • Superpneumarary arches 5. Double Aortic Arch 6. Persistent Fifth AA 7. Interrupted Aortic Arch 8. Anomalous origin of PA branches and other AA anomalies
2. Abnormal L Aortic Arch • L AA with retroesophageal R SCA • L AA with R Desc Ao & R ductus
2.1 L AA with retroesophageal R SCA • Most common arch anomaly – 0.5% of general population • Higher incidence in Downs with CHD – 38% • Mostly asymptomatic
2.1 L AA with retroesophageal R SCA • Diagnosis • Echo/angio • Branch sizes of 1=2, 3=4 • 1st – no bifurcation, goes to R • 2nd,3rd – to L, non bifurcating • 4th – towards R, disappear behind trachea
2.1 L AA with retroesophageal R SCA • Ba oesophagography • Small filling defect slanting up and R • MRI
2.2 L AA with R Desc Ao & R ductus • Branching pattern similar to previous • Rare • Arch – retro-oesophageal • Desc Ao connected to PA by R ductus ring
2.2 L AA with R Desc Ao & R ductus • Diagnosis • Suspect when symps of vascular ring + L aortic arch present • CxR • L Ao A + R upper desc. Ao (adults)
2.2 L AA with R Desc Ao & R ductus • Diagnosis • Ba oesophagography • Large indentation directed up and L • DD – R Ao A with retro-oesophageal diverticulum • Angiography, MRI
2.2 L AA with R Desc Ao & R ductus • Rx – R thoracotomy & division of ring
Anatomical Categories • Abnormalities of branching • Normal L Aortic Arch & Variants • Abnormal L Aortic Arch • Abnormalities of arch position 3. R Aortic Arch 4. Cervical Aortic Arch • Superpneumarary arches 5. Double Aortic Arch 6. Persistent Fifth AA 7. Interrupted Aortic Arch 8. Anomalous origin of PA branches and other AA anomalies
3. R Aortic Arch • Definition • Single aortic arch that crosses over the R main bronchus passing to the R of the trachea
3. R Aortic Arch Major types • R AA with mirror image branching • R AA with retro-oesophageal L SCA • R AA with retro-oesophageal diverticulum • R AA with L descending aorta
3. R Aortic Arch • 13- 34% of TOF have RAA • Incidence in Truncus Arteriosus > that of TOF • 8% of DTGA, 16% of TGA+VSD+PS have RAA
3.1 RAA with Mirror Image Branching • Almost always ass. with congenital intracardiac disease • Conotruncal anomalies – TOF, TA, TGA, DORV, LTGA, PA with RV aorta • Other lesions – VSD, PA with IVS • Ductus is commonly L sided - attached to L innom. A. – no vascular ring
3.1 RAA with Mirror Image Branching • Diagnosis • Usually no retro-oesophageal compression/ vascular ring • Echo/Angio • Distinctive branching pattern • CxR/ Ba oesophagography • R indentation of trachea/oesophagus • Treatment • RAA only - No Rx needed
3.1 RAA with Mirror Image Branching • Variant – • L ductus to RE diverticulum from R Desc Ao • Vascular ring • No arch vv from diverticulum (Rarely true mirror image of normal – L ductus disappear and R 6th arch continue as ductus)
3.2 RAA with Retro-oesophageal diverticulum (Of Kommerell) • vascular ring+ • Many asymptomatic, in most no other heart defect
3.2 RAA with Retro-oesophageal diverticulum (Of Kommerell) • Diagnosis • Presentation – vascular ring • +CxR – R AA ? RE Div of Com • Ba Oesophagogram • Echo • Angio – charact branching pattern, abrupt change in caliber from diverticulum to SCA • MRI
3.2 RAA with Retro-oesophageal diverticulum (Of Kommerell) • Rx • Symptomatic – Sx division of ligamentum (L thoracotomy/ Median sternotomy) • If resp symps/ dysphagia – resection of entire diverticulum (R thoracotomy)
3.3 R AA with Retro-oesophageal L SCA • Loss of L 6th ductal arch and persistence of R 6th • No vascular ring • Smaller posterior indentation of Oesophagus • Rx not needed (no ring) except for ass anomalies