Download
1 / 15
281 likes | 1.22k Views
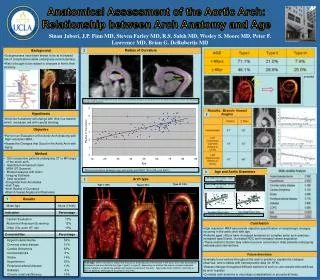
Interrupted Aortic Arch. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Interrupted Aortic Arch. 1. Definition A complete luminal & anatomic discontinuity between the two segments of the aortic arch 2. History

E N D
Interrupted Aortic Arch Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Interrupted Aortic Arch • 1. Definition • A complete luminal & anatomic discontinuity between • the two segments of the aortic arch • 2. History • Steidely : 1st description in 1778 • Celoria and Patton : A, B, C type in 1959 • Samson : 1st successful operation • in 1955 • 3. Classification • Type A (40%), Type B (55%), Type C ( 5%)
Pathophysiology of IAA • Luminal interruption between the ascending and descending aorta is found, and distal blood flow is dependent on a patent ductus arteriosus. • Spontaneous ductal closure results in systemic hypoperfusion, metabolic acidosis , and end-organ failure • Associated cardiac anomalies are common, particularly a nonrestrictive VSD, and IAA comprises less than 1% of all CHD
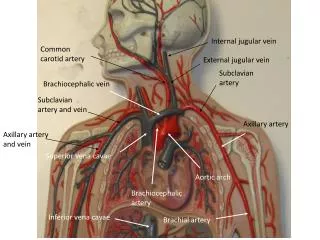
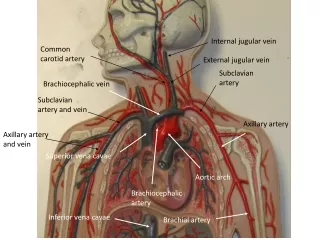
Embryonic Origin of Aortic Arch • 1. Ascending aorta : Embryonic conotruncus • 2. Proximal arch : Embryonic aortic sac • 3. Distal arch : 4th embryonic aortic arch • 4. Isthmus : Junction of 6th embryonic • arch with left dorsal aorta & • 4th embryonic aortic arch
Morphology of IAA • 1. Aortic arch • * Anomalies of brachiocephalic vessels are frequent. • * Rare interruption in right aortic arch • 2. Left ventricular outflow anomalies • * Bicuspid in 30-50% • * Aortic and subaortic stenosis • * Aortic ring is frequently small • 3. Coexisting cardiac anomalies • * PDA is almost always • * Large VSD is nearly always • * Truncus arteriosus, aortopulmonary window • 4. Associated syndrome • * DiGeorge’s syndrome (absence of thymic tissue) • - hypocalcemia & immunologic problem (Type B)
Clinical Features in IAA • 1. Clinical features • * Critically ill neonate in severe CHF • * Cardiac murmurs are not specific. • * Closing PDA ; anuria & metabolic acidosis • 2. Natural History • * 1~4% of CHD in autopsy ( 1.3% of CHD in infancy ) • * Median age of death : 4~10 days • * 90% death in the 1st. year even though PDA • * Pulmonary vascular disease after one year
DiGeorge’s Syndrome • 1. Complete type • * dysmorphic facial feature • : hypertelorism, carp-shaped mouth, • micrognathia, notched ear pinnae • * hypocalcemia • * Low T lymphocyte CD4 • * IAA • 2. Partial type • * Facial feature with hypocalcemia and IAA in • the absence of any deficit of CD4 T lymphocyte
Berry Syndrome • Interrupted aortic arch • Distal aortopulmonary septal defect • RPA from ascending aorta • Intact ventricular septum
Operation of IAA • 1. Indication • * Urgent operation is advisable, preferably • by a one-stage. • 2. Technique • * Direct anastomosis (open or non-open technique) • * Interposition of graft • * One stage repair • Median sternotomy and circulatory arrest, • IAA and associated anomaly repair
Early Operative Results of IAA Mortality & morbidity 1) Early death Acute or subacute heart failure without or with multisystem failure. One stage repair : under 10% IAA repair & second repair : 12-47% mortality • 2) Late • Survival : good • Aortic anastomotic narrowing • Development of subaortic stenosis (44-85%)
Operative Results of IAA • 1. Survival • Early death • Time-related survival • 2. Modes of death • 3. Incremental risk factors for premature death • 1) Coexisting cardiac anomalies • 2) Location of interruption • 3) Preoperative condition • 4) Earlier date of operation • 4. Left ventricular outflow obstruction • 5. Persistent or redeveloped aortic arch obstruction