Download
1 / 116
1.16k likes | 1.24k Views
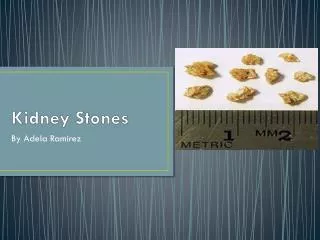
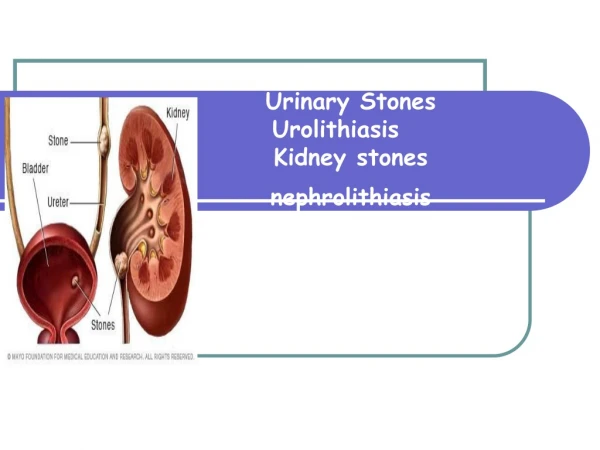
Urinary Stones. Assoc.Prof.Dr Hakan Koyuncu Yeditepe University Medical Faculty Urology Department. Definition. Stones of the urinary system are collections of crystalloid products and may also be made out of organic matrix creating polycrystalized hard structures

E N D
Urinary Stones Assoc.Prof.Dr Hakan Koyuncu Yeditepe University Medical Faculty Urology Department
Definition • Stones of the urinary system are collections of crystalloid products and may also be made out of organic matrix creating polycrystalized hard structures • 3rd most common pathology of the urinary system after prostate pathologies and urinary tract infections • Multiple complex factors play a role in stone formation and occur after a series of actions
EPIDEMIOLOGY and ETIOLOGY • Prevelance %4-20 • Prevelance in Turkey %15-18 • Age 30-50y • M:F 2:1 • Risk for men is around % 12 and for women around% 5 • Race white > black • Climate (high in Mediterranean climate)
Protein , Carbohydrate or Oxcalate rich Diet • Alcohol (increase uric acid in blood and Ca/P in urine) • Inheritance (Primary hyperoxaluria ,cystinuria ,xantinuria) hastalığın insidans ve prevalansını etkileyen faktörlerdir. • Family History (1. derece akrabada varsa risk 3 kata yakın daha fazla ve erken nüks olasılığı yüksek. Önceden taş hastalığı geçiren olguların yaklaşık % 50-70 kadarında 7-10 yıl içerisinde yeniden taş oluşabilir. • DIET + HEREDITY + PHYSICAL ACTIVITY
↑Fluid Intake ↓stone formation • Citrate,Mg , F, Sulfate levels in urine FEMALE ↑ Citrate levels in urine = ↓ stone formation
Medications( overuse ) • Antihypertensive triamters, diazide • Sulfadiazine,acetazolamide • Hypertension(↑Ca uria) • Crohns disease , short gut syndrome,UC, radiation and chronic diarrhea
Exceptionalcircumstances; • Kidney transplant • Pregnancy • Obesity • Medullaryspongekidney, polycystickidneydisease, Horse-shoekidney, ectopickidney • Renal tubularacidosis(typ 1) • Infections • Tumors • Calyxdiverticulums
ETHIOPATHOGENESIS Stone formationoccurs in 3 steps
Supersaturation – Crystalization • If an element, able to crystalize, is added to a fluid of a certain temperature and pH : • it remains in its melted form to a certain temperature. • It may start breaking down as if its mass increases and the fluid gets saturated further. • the “ Solubility Product “ is formed as breaking down starts • the “ Formation Product” is the point at which crystalization occurs in supersaturated urine • The level before SP is called stable zone and the stage between SP-FP is called metastable region
Labile supersaturation Spontaneous nucleation FP homogeneous nucleation Heterogeneous nucleation Metastable supersaturation FP heterogeneous nucleation Solubility Product Undersaturation No nucleation No nucleation
no crystal nucleus is formed during Stable zone, but if, they don‘t grow • Formed nucleus may grow during Metastable part • Sponatneous crytsal nucleus may get formed during FP stage • Crystal nucleation can be heterogenous or homogenous • Crystal spheres in urine may get aggregated and grow • Not every saturated urine causes nucleation. Hence this theory alone is not sufficent for stone formation
Absence of Urine Inhibitors • Organic structures: High mollecular glycoproteins (GAG), Matrix-A , SH bond containing urommucoids, Alanin , Cytrates • Cytrates show the highest inhibitory effect • Inorganic structures: Phosphates ,Pyrophosphates , Orthophosphates , Magnesium , Zinc • Orthophosphates transforming into Pyrophosphates in prophylactic treatment
Matrix Nucleation • Matrix is made from Proximal Tubular epithelial cells. • Includes matrix ,protein,hexane and hexamines • Matrix has an inhibitory- effect by preventing crystal growth and aggregation • On the other hand 2-10% of stones contain Matrix • Microlites produced on the matrix of the tubular lumen –Idiopathic Ca stone diseases
Urinary foreign bodies ,epithelial breakdowns ,erythrosites , leukocytes ,Alb, alfa-1, alfa-2 globulin –like structures act as matrix and may lead to stone formation. • Substance A – immunological component that initiates crytal aggregation Stone specifig Ag
Possible Matrix Promoters • Cell membrane particles • Cellular breakdown product • Phospholipids • Lipids • Macrmolecules • Heterogen crystallin substances
Epitaxy • Crystal growth may stop after accumulation of a certain substance with increasing urinary saturation. Substance formed due to the secondary risk factors may accumulate over the primary crystalsdifferent inner and outer layers • Ex.Ca oxalate substance holding onto uric acid crystals by epitaxy.Cystin does not accumulate on other nuclei.
Combined Theory • None of the above mentioned theories are enough alone but the combination of theories are much more effective in stone formation.
Predisposing Factors • pH changes in urine • UTI • Congenital anomalies • Urostasis • Calcification in Kidney • Urinary tract foreign bodies,fistulas ,tumors,necrotic tissue segments
Crystaluria • Crystal formed in the Papilla reaches bladder in 10-15 minute and excreated in 3-6 hr. • Physiological crystaluria is common and normal process.
Genetic • Cystin • Xantine • 2-8 Dihydroxyadenin • Drug related
% 70-88 Ca containing stones (Ca oxalate(%36-70),Ca phosphate(apatite)(%6-20) • % 6-20 Infection (struvite) (magnesium ammonium phosphate) • % 6-17 Uric acid • % 0,5-3 Cystin • % 11-31 Mixed • Pt can have multiple types of stones at once
Ca stones • 70-90% of all kidney stones • Mostly found as mixed • 80% of all stones are only or mainly made of Ca Oxalate • Seen in inmobile patients • Increase in Ca ,uric acid and oxalate and decrease in citrate (hypercalciuria,hyperoxalouria,hyperuricoseuria,hypocytraturia)
Hypercalciuria • Less than 275 mg/24 hr of Ca is excreated (Healthy men having 1 gr Ca per day),250 mg in women • Ca in urine <4 mg/kg/24 hr • Ca in urine > 4 mg/kg/24 hr Hypercalciuria • Idiopathic Ca stones 50-70% has Hypercalciuria
Hypercalciuria • 1-Absorptive • 2-Renal • 3-Resorptive • 4-Other
Absorptive • Normal Ca intake 900-1000mg/day • 1/3 of it absorbed from Intestines and 150-2000mg excreated from urine.Most common Hypercalciuria type. 50-60% of Ca oxalate. • Intestinal Hyperabsorbtion is the main point .Increased response to the Vit D leads to over absorbtion of Ca increased Ca in circulation ,increased Renal filtration Parathyroid functions are suppressed
Absorptive Hypercalciuria ; • Type I : Hypercalciuria w/ low Ca Diet • Type II : Hypercalciuria w/ high Ca Diet • Type III : Increased Vit Dsynthesis due to Renal Phosphate leakage
Renal Hypercalciuria • Primary anomaly low Ca absorbtion from Renal Tubules( 10% of all stone formations ) • ↓Ca (serum) PTH stimulation • Secondary HyperParathyroidism • ↑PTH in Bone Ca mobilization D3 renal synthesis and Intestinal Ca absorbtion ↑Hypercalciuria
Resorptive Hypercalciuria • Primary HyperPTH 4% of all stone formations • PTHtransport of Ca from bone to bloodby Vit D increased intestinal absorbtion • Increased Ca in blood: • Hypercalcemia • Hypercalciuria • Hypophosphatemia • Hyperphosphaturia • Multiple stones ,Nephrocalcinosis,Ca deposition in Tubules
Absoptive RENALHypercalciuria Resorptive • SERUM: Ca:N • Secondary PTH HIGH • SERUM Ca: N • PTH:NORMAL or Low • SERUM Ca: N • Primary PTH: HIGH
Hyperoxaluria • 50% of Oxalate is destructed by intestinal bacterias • 25% excreated with feces • 15-20%absorbed by intestines and excreated by urine • 15% of Urinary oxalate is absorbed by GIS ,80% is endogenic(ascorbic acid 40%-glicooxalic acid 60%)
Hyperoxalcuria : >40 mg/day oxalate excretion through urine • Calcium is a bigger risk factor in stone format • Oxalate reabsorbtion in the colon may increase which could be caused by IBD, small bowel resection or jejuno-ileal by-pass. • In malabsorbtion calcium is low due to it‘s increased binding potential with lipds hence oxalate binding potential with calcium decreases and causes oxalate to be reabsorbed more.
Hyperoxaluria has 3 types • Primary (genetic) • Enteric • Dietary
Primary hyperoxaluria • Autosomal recessive Nephrocalcinosis • < 40 y kidneyfailure • Tip I Glyoxalate carboligase deficiency(2.chromosome AGXT gene mutation) • Tip II D-glycerate dehydrogenase deficiency (9. chromosome GRHPR gene mutation) • ↑ Oxalate in urine , vessel walls and soft tissue
Enteric hyperoxaluria • Low Ca++ causing decreased CaOx complex formation in bowel • Insufficient calcium intake • Ca gets bined with bile and lipids excretion • Absorption provocated by bile and lipid acids increasing transport of oxalate in bowel • Increased reabsorbtion of oxalate by unknown causes (vegetables with green leaves,lemon, dark grapes,tea,cocoa,nuts,coffee contain high amounts of oxalate)
Other hyperoxaluria • Ethylenglycol or metoxyfloranpoisoning • High dose intakeofascorbicacid( > 5 mg/gün) • Lack ofbacteriabreaking down oxalate in bowel ( OxalobacterFormigenes)
Hypocytraturia • Cytrates are the most important inhibitors in stone formation. Decreases calcium saturation by forming soluble complexes with calcium salts • Important factor in organic stone formation and idiopathic stone formations • Often occurs in patients withrenal tubular acidosistype 1, thiazide treatment & chronic diarrhea • Diet and oral medical treatment can cause relapse
Hyperuricosuria • High intake of purine containing nourishment • Increased endogenous uric acid production • Urine pH <5.5 • Uric acid in urine >750 mg in 24 hours
Hypomagnezuria • Potent inhibitor • Mostly related to oral intake
Uric acid stones • More common in high ptotein intake • Final product of purine metabolism • Uric acid is turned into allanoine breaks down in water no stone production
Mechanisms: 1) Decrease of urinary pH 2) Hyperuricosuroa 3) 1+2 • Uric acid is insoluble • Only half of it can be ionized in urine with a pH 5.75 • if pH is 5 50 mg/dl uric acid but in pH 7 urine it‘s 200 mg/dl • If urine is acidic increased risk
Meat, fish etc • Uricouric drug intake (probeneside, ascorbic acid...) • alcoholism • obesity • dehydration • increased acidic drinks and foods • starving • Gout disease
URIC ACID STONES ARE NON-OPAQUE NOT VISIBLE ON X-RAY • Low urine pH • Uric acid >750 mg/day • STONE ANALYSIS definite diagnosis
Infective stones(STRUVITE) • 10-15% of all stones • More common in children and women • Mixture of magnesium amoniumphosphate and carbonate apatite Struvite Kristalleri
2 main mechanisms • 1) Infection caused by bacteria breaking down urea (containing urea) • 2) Urine amonium, phosphate and carbonate have to be saturated No supersaturation without infection!