Download
1 / 49
500 likes | 604 Views
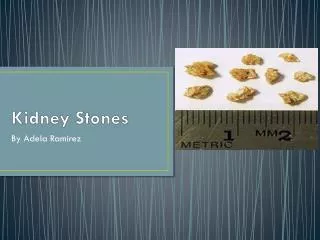
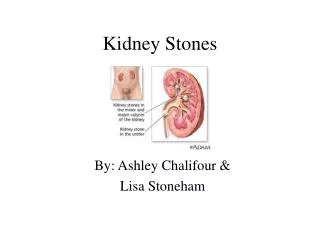
Urinary Stones Urolithiasis Kidney stones nephrolithiasis. Kidney stones. Kidney stones (renal calculi)

E N D
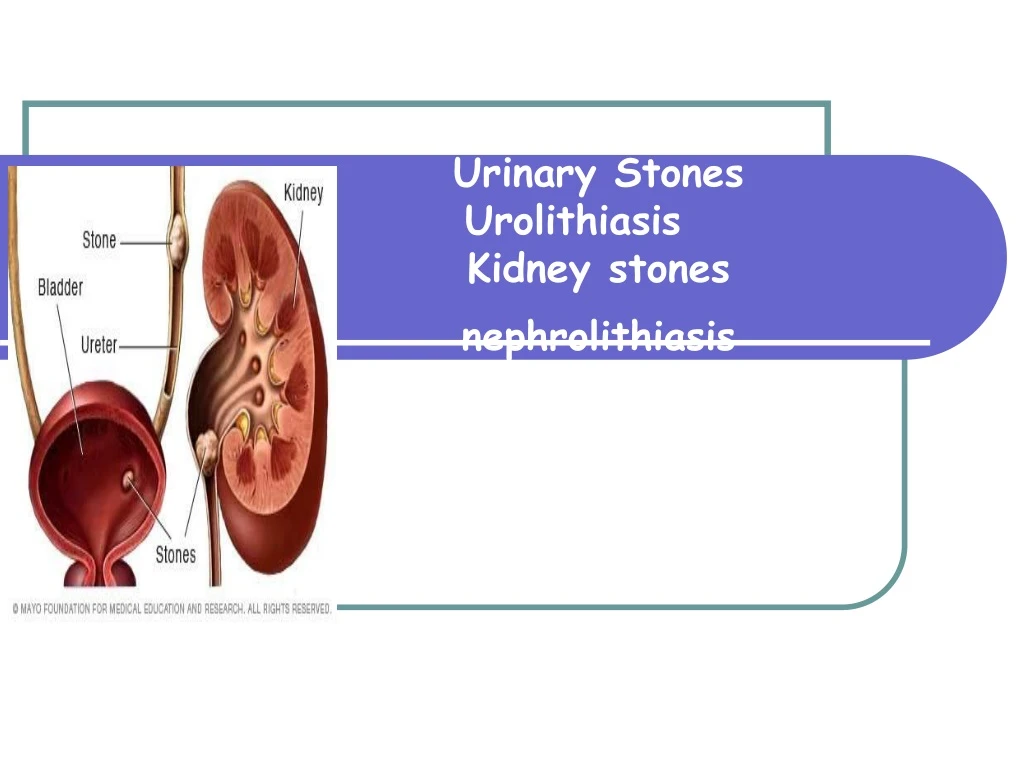
Urinary Stones Urolithiasis Kidney stones nephrolithiasis
Kidney stones Kidney stones (renal calculi) Aadalah batu yang terbentuk di dlm tub ginjal dan biasanya tersusun dari produk metabolisme yang difiltrasi glomerulus yang biasanya disebabkan karena konsentrasinya mendekati ambang maksimumnya.
Kidney stones Nephrolithiasis : adanya batu di dalam ginjal Urolithiasis : adanya / ditemukannya batu di dlm traktus urinarius
Stones form in the urinary tract • Ada tiga cara : • 1. terbentuknya kristalkristal • 2. kristal2 tsb beragregasi satu sama lain • 3. menjadi batu kristal yg ckp besar utk memblok saluran urinari
Conditions favouring kidney stones formation 1. Konsentrasi zat terlarut yang harus melalui filtrasi di glomerulus di atas ambang batasnya 2. Perubahan pH urine. 3. Menahan Urin 4. Kurangnya inhibitor/faktor penghambat yg berperan dlm pembentukan batu ginjal
Conditions favouring kidney stones formation 1. Konsentrasi urine meningkat menyebabkan: - volume urine (dengan fungsi ginjal normal) • - Restricted fluid intake • - meningkatan kehilangan cairan pada periode yang panjang
- ekskresi metabolik menyebabkan peningkatan pembtkan batu ginjal • * volume plasma volume ( yang bs meningkatkan laju filtrasi glomerulus) • * reabsopsi tubulus dari hasil filtrasi
Conditions favouring kidney stones formation 2- perubahan pH urine - often due to bacterial infection - precipitation of different salts at different pH: • * A persistently acidic urine • promotes uric acid precipitation • * A persistently alkaline urine (due to upper urinary tract infection) promotes Mg Ammonium Phosphate crystals (Struvite stones)
Conditions favouring kidney stones formation 3. Urinary stagnation: - Due to obstruction of urinary outflow 4- Lack of normal inhibitors in urine - Inhibitors of stone formation: e.g.: Citrates Pyrophosphate Glycoproteins
Constituents of Kidney Stones 1. garam kalsium 2. asam urat 3. magnesium amonium fosfat 4. Batu kristal Cystine stones 5. lain2 (Xantihine,dll)
Stones – Chemical Constituents Whewelite – Calcium Oxalate Monohydrate – CaC2O4-H2O Weddelite - Calcium Oxalate dihydrate – CaC2O4-2H2O Brushite – Calcium Hydrogen phosphate dihydrate – CaHPO4 2H2O Whitlockite - TriCalcium Phosphate – Ca2(PO4)2 Struvite – Magnesium Ammonium hexahydrate – MgNH4PO4-6H2O
Uncommon Stones XANTHINE STONES – (kelainan autosomal resesif, defisiensi xanthine oxidase akan memicu xanthinuria) DIHYDROXYADENINE STONE – ( Defisiensi enzim adenin fosforibosil tranferase)
Uncommon Stones SlLICATE STONES – jarang terjadi pada manusia (kelebihan intake antasida yang mengandung Mg trisilicat) MATRIX - Infeksi oleh Proteus
Uncommon Stones TRIAMTERENE - terapi untuk menjaga kadar Na tetap rendah, diberikan utk mencegah penumpukan cairan (edema) pada penderita gagal jantung – penggunaan anti hipertensi dengan hidroklorotiazid – bagian potassium. Umumnya ditemukan sebagai inti pada Ca oksalat atau kalkulus asam urat
Uncommon Stones Indinavir Stones - Drug to treat AIDS (4 to13%) Ephedrine or Guifenesin – Cough medicine - Radiolucent
Constituents of Kidney Stones: 1-Stones of calcium salts • * 80% of pasien dengan nephrolithiasis membentuk batu kalsium dari: • - paling srg: Ca-Oxalate • - jarang dari: Ca-Phosphate • * Type of salt depends on: - pH urin • - asupan oksalate
Constituents of Kidney Stones:1-Stones of calcium salts(cont.) karakteristik: - putih, keras dan radioopak - Ca-Oxalate: lebih kecil, terkumpul di ureter - Ca-Phosphate: staghorn, di renal pelvis (besar)
Constituents of Kidney Stones:1-Stones of calcium salts (cont.) Beberapapenyebabpembentukanbatuginjalkalsium:: 1- Hypercalciuria: Defined as daily urinary Ca excretion >6.2 mmol in ♀ & >7.5 mmol in ♂ - due to hypercalcemia (most often due to 1aryhyperparathyroism) - sometimes, Ca++ salts stones are found with no hypercalcemia
2- Hyperoxaluria (more important ) - favours formation of calcium oxalates (even with no hypercalciuria) - causes: * exogenous (diet rich in oxalate ) * absorption (in fat malabsorption) * 1aryhyperoxaluria: inborn errors , in childhood , urinary oxalates > 400 mmol/24 hours
Increased intestinal absorption of calcium (absorptive hypercalciuria), • excessive hormone levels hyperparathyroidism • renal calcium leak (kidney defect that causes excessive calcium to enter the urine) • Prolonged inactivity also increases urinary calcium and may cause stones. • Renal tubular acidosis (inherited condition in which the kidneys are unable to excrete acid) significantly reduces urinary citrate and total acid levels and can lead to stone formation.
Constituents of Kidney Stones:1-Stones of calcium salts (cont.) Conservative lines of treatment: * Treatment of primary condition (i.e. Infection, hypercalcemia, hyperoxaluria) * Reducing oxalates in diet (it is not recommended to reduce calcium in diet) * Fluid intake (if no glomerular failure). *Acidification of urine (as ppt. is favoured by alkaline conditions)
Constituents of Kidney Stones:2-Uric acid stones - ~ 8%of renal stones contains uric acid • - may be associated with hyperuricemia (with • or without clinical gout) • -Characteristics: * small, friable & yellowish * may form staghorn (if big) * radiolucent (can’t be seen be plain X-ray) * visualized by ultrasonography or I.V. Pyelogram
Uric Acid Stones • Digestion produces uric acid. • If the acid level in the urine is high or too much acid is excreted, the uric acid may not dissolve and uric acid stones may form. • They are not visible on X-rays. • Patients with gout often develop these stones.
- Uric acid stones are more often caused by low urine pH. - Even relatively high uric acid excretion will not be associated with uric acid stone formation if the urine pH is alkaline. Therefore, prevention of uric acid stones relies on alkalinization of the urine with citrate. Potassium citrate Is also used in kidney stone prevention-
Cont. • Genetics may play a role in the development of uric acid stones, which are more common in men. • Approximately 10% of patients with kidney stone disease develop this type of stone.
Constituents of Kidney Stones:2-Uric acid stones, (Cont.) Treatment: - Treatment of cause of hyperuricemia - purine-rich diet - Alkalinzation of urine (e.g. by potassium citrate) - fluid intake
Constituents of Kidney Stones:3- Magnesium ammonium phosphate stones * ~ 10% of all renal stones * With chronic urinary tract infection (by urease splitting organisms as Proteus species ammonia production from urea) * Alkaline urine pH (> 7.0)
Struvite Stones • Also called an infection stone, develops when a urinary tract infection (e.g., bladder infection) affects the chemical balance of the urine. • Bacteria in the urinary tract release chemicals that neutralize acid in the urine, which enables bacteria to grow more quickly and promotes struvite stone development.
Cont. • They are capable of splitting urea into ammonia, decreasing the acidity of the urine and resulting in favorable conditions for the formation of struvite stones. • Organisms which alkalinize the urine can cause struvite stones to form. • Struvite stones are more common in women.
-The stones usually develop as jagged • structures called "staghorns" and can grow to be quite large.
Treatment: * Aggressive prevention & treatment of the cause (urinary tract infection) * Urine acidification * Fluid intake * It may require complete stone removal (percutaneous nephrolithotomy) • * Aggressive prevention & treatment of • future urinary tract infection
Constituents of Kidney Stones:4- cystine stones • Cystine is an amino acid. • Some people inherit a rare, congenital condition that results in large amounts of cystine in the urine (cystinuria) causes cystine stones that are difficult to treat and requires life-long therapy. *
Cystine Stones * Rare * occurs in cases of homozygous cystinuria (inborn error of amino acid metabolism) • * Soluble in alkaline urine (precipitates by • acidic urine) Treatment: - fluid intake - Alkalinzation of urine - Penicillamine
The key features to the formation of stones • Family history, • Age of onset, • Fluid intake pattern, • Diet, medications, • History of infections. • Certain stone formation has a genetic predisposition
- Some an autosomal recessive pattern, including cystinuria and primary hyperoxaluria, - Some have an autosomal dominant pattern such as renal tubular acidosis (RTA) or the syndrome of idiopathic calcium oxalate urolithiasis. • -
Causes and Risk Factors • A low level of citrate is a risk factor for hypocitraturia. • Congenital kidney defect that may increase urinary calcium loss and stone formation (medullary sponge kidney) • Excessive parathyroid hormone, which causes calcium loss (hyperparathyroidism)
Gout (caused by excessive uric acid in the blood) • High blood pressure ( hypertension) • Inflammation of the colon that causes chronic diarrhea, dehydration, and chemical imbalances (colitis) • Sodium (hypernatremia)
Inherited condition in which the kidneys are unable to excrete acid (renal tubular acidosis) • Painful joint inflammation (arthritis) • Urinary tract infectious (affect kidney function)
- A diet high in sodium, fats, meat, and sugar, and low in fiber, vegetable protein, and unrefined carbohydrates increases the risk for renal stone disease. - High doses of vitamin C (i.e., more than 500 mg per day) can result in high levels of oxalate in the urine (hyperoxaluria) and increase the risk for kidney stones.
Oxalate is found in berries, vegetables (e.g., green beans, beets, spinach, squash, tomatoes), nuts, chocolate, and tea. • Stone formers should limit their intake of cranberries, which contain a moderate amount of oxalate.
Certain foods may increase the risk of stones - spinach, rhubarb, chocolate, peanuts, cocoa, tomato juice, grapefruit juice, apple juice, soda (acidic and contains phosphorus), and berries (high levels of oxalate). Other drinks are associated with decreased risk of stones, - wine, lemonade and orange juice (rich in citrate -- a stone inhibitor
Allopurinol reduces calcium stone formation Thiazides are the medical therapy of choice for most cases of hypercalciuria Cellulose supplements have also shown potential for reducing kidney stones caused by hypercalciuria