Download
1 / 37
370 likes | 388 Views
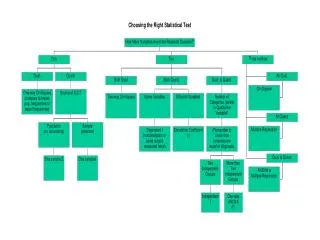
Learn how to choose an HIV testing strategy, understand sensitivity and specificity, and calculate predictive values. Explore different testing options and quality control measures for accurate results.

E N D
Unit 5: Choosing an HIV Test #3-5-1
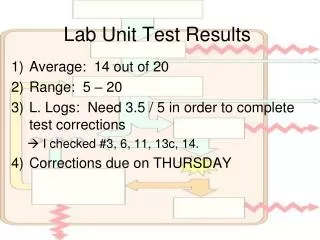
Warm Up Questions: Instructions • Take five minutes now to try the Unit 5 warm up questions in your manual. • Please do not compare answers with other participants. • Your answers will not be collected or graded. • We will review your answers at the end of the unit. #3-5-2
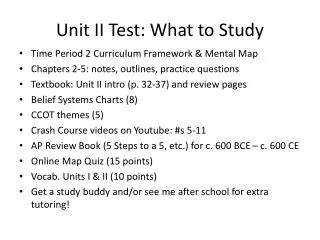
What You Will Learn • By the end of this unit you should be able to: • describe the advantages and disadvantages of different HIV testing options • describe how to choose a strategy for HIV testing #3-5-3
What You Will Learn, Cont. • By the end of this unit you should be able to: • understand the difference between sensitivity and specificity of a laboratory test • identify the phases of the testing process, and what quality control and quality assurance programmes should be implemented in each phase #3-5-4
Selecting an HIV Antibody Test • Currently a wide range of different HIV antibody tests are available, including: • Conventional enzyme immunoassay (EIA) • Rapid tests #3-5-5
Selecting an HIV Testing Algorithm • UNAIDS and WHO recommend three criteria for choosing and HIV testing algorythm or strategy: • objective of the test (surveillance, blood screening, etc) • sensitivity and specificity of the test(s) being used • HIV prevalence in the population being tested #3-5-7
Table 5.2. Selection of HIV Testing Algorithms for Surveillance #3-5-8
Sensitivity and Specificity • Sensitivity refers to the ability of a test to detect all persons with a disease: • Specificity refers to a test’s ability to detect all persons who do not have a disease: #3-5-9
Positive and Negative Predictive Value • Positive predictive value: proportion of positive tests that identify people who truly have a disease • The more frequent a disease is in a population, the higher the positive predictive value of a test is. • Negative predictive value: proportion of negative tests that identify people who truly do not have a disease #3-5-10
Disease Total Test result Present Absent Positive a b a + b Negative c d c + d Total a + c b + d a + b + c + d Table 5.3. Guide for Calculating Sensitivity and Specificity #3-5-11
Testing Strategy 1 • Requires one test • For use in diagnostic testing in populations with an HIV prevalence >30% among persons with clinical signs or symptoms of HIV infection • For use in blood screening, for all populations regardless of the estimated prevalence in population being tested #3-5-12
Testing Strategy 1, Cont. • For use in surveillance testing in populations with an HIV prevalence >10% (for example, unlinked anonymous testing for surveillance among pregnant women at ANCs) • No results are provided #3-5-13
Testing Strategy 2 • Requires up to two tests • For use in diagnostic testing in populations with an HIV prevalence ≤ 30% among persons with clinical signs or symptoms of HIV infection or >10% among persons with no such signs or symptoms #3-5-14
Testing Strategy 2, Cont. • For use in surveillance testing in populations with an HIV prevalence ≤ 10% (for example, unlinked anonymous testing for surveillance among pregnant women at ANCs or patients at STI clinics) • No results are provided #3-5-15
Figures 5.1 and 5.2. Strategies for HIV Testing Strategy 1 Strategy 2 #3-5-16
Selection of HIV Testing Technologies • Decide which testing format to use: • an enzyme linked immunoassay (EIA), • rapid EIA testing, or • a combination of the two • Conditions to consider include: • laboratory infrastructure • availability of skilled laboratory personnel • existence of quality assurance and control measures #3-5-17
Laboratory Testing • The laboratory tests now in use have sensitivities and specificities of 99% or more. • In sub-Saharan Africa, HIV tests performed must be able to detect the presence of antibodies to both HIV-1 and HIV-2. • An additional test is required to distinguish between HIV-1 and HIV-2. #3-5-18
Quality Control • Quality control: process for running the specimens (such as using positive and negative controls), done in the lab facility itself • To verify test device is accurate, external positive and negative controls must be tested. • The test kit manufacturer or a reference laboratory can provide these controls. • Positive controls: specimens known to be positive • Negative controls: are specimens known to be negative #3-5-19
Quality Assurance • Quality assurance: process for comparing results obtained for a specific test with other tests done on the same specimen, done by the lab itself or by outside reference laboratory • Laboratories should monitor and assess quality during three phases of the testing process: • pre-analytical: activities that occur before a specimen is tested • analytical: the actual testing of the specimen • post-analytical: activities done after a specimen has been tested #3-5-20
Table 5.5. Quality Assurance: Pre-Analytical Phase • Training • Laboratory safety • Number of trained personnel available and capable of performing HIV testing • Specimen collection, labelling and transport conditions • Deciding on handling of specimens before testing #3-5-21
Table 5.5. Quality Assurance: Pre-Analytical Phase, Cont. • Deciding on the sources and types of specimens to be tested • Deciding on the number of specimens tested • Selection of test kits • Expiration dates of test kits. Kits need to be used before expiration dates. Older kits should be used before newer kits. • HIV test kit reagents. Reagents must be stored at the appropriate temperature as specified by the manufacturer. #3-5-22
Table 5.5. Quality Assurance:Analytical Phase • Specimen processing and storage • Written procedure manual • Reagent preparation • Testing performance • Performance and maintenance of equipment • Correct use of reagents • Inclusion of internal quality controls in test kits • Quality control monitoring procedure #3-5-23
Table 5.5. Quality Assurance: Post-Analytical Phase • Interpreting results • Transcribing results, such as recording results on the correct identifier code • Entering data into the tracking system (computer or hard copy) • Maintaining records • Reviewing quality control #3-5-24
Internal Quality Assurance • Internal quality assurance is meant to allow laboratory technicians to check their performance for themselves: • An aliquot of every twentieth negative and every fifth positive specimen is put aside. • Once there are sufficient stored aliquots, stored specimens are tested a second time. • Lab technicians compare initial results and results of re-testing to monitor reliability of techniques. #3-5-25
External Quality Assurance • Countries should require that all laboratories at all levels participate in an external quality assurance programme. • This may be instituted either by a national or international reference laboratory. • Proficiency testing should be done 1-2 times a year. #3-5-26
External Quality Assurance, Cont. • In areas with limited infrastructure, labs can prepare a dried blood spot on filter paper to be tested at the national reference laboratory. • External quality assurance for national reference laboratory should be provided by an independent laboratory or one of WHO’s regional quality assurance programmes. #3-5-27
External Quality Assurance Procedure • Procedure: • National reference laboratory sends to all participating laboratories a proficiency panel of 6 specimens to identify as HIV- or HIV+. • Panels are tested at local laboratories in the same way as they routinely test their specimens for HIV. • Local laboratories report their findings to the reference laboratory, which collates results and provides feedback. #3-5-28
Warm Up Review • Take a few minutes now to look back at your answers to the warm up questions at the beginning of the unit. • Make any changes you want to. • We will discuss the questions and answers in a few minutes. #3-5-29
Answers to Warm Up Questions • Which of the following is a factor in the decision to select an HIV testing strategy? • sensitivity and specificity of test being used • objective of the test • HIV prevalence in the population being tested • all of the above #3-5-30
_b_ pre-analytical _c_ analytical _a_ post-analytical interpreting results, entering data into tracking system, reviewing quality control training, laboratory safety, selection of test kits specimen processing and storage, analysis of testing performance, reagent preparation Answers to Warm Up Questions, Cont. 2. Match each phase of the HIV testing process with the components it includes: #3-5-31
Answers to Warm Up Questions, Cont. 3. The process by which reference specimens are tested externally to assure accuracy of a technician’s or laboratory’s performance is known as: • quality control • quality assurance • quality performance • none of the above #3-5-32
Small Group Discussion: Instructions • Get into small groups to discuss these questions. • Choose a speaker for your group who will report back to the class. • Take 15 minutes for this exercise. #3-5-33
Small Group Reports • Select one member from your group to present your answers. • Discuss with the rest of the class. #3-5-34
Case Study: Instructions • Try this case study individually. • We’ll discuss the answers in class. #3-5-35
Case Study Review • Follow along as we go over the case study in class. • Discuss your answers with the rest of the class. #3-5-36
Questions, Process Check • Do you have any questions on the information we just covered? • Are you happy with how we worked on Unit 5? • Do you want to try something different that will help the group? #3-5-37