Download
1 / 43
471 likes | 814 Views
The Aging Eye. Dr. Desinee Drakulich. Disclosure Statement. I have no affiliation or get paid by any of the companies who’s products I discussed in this lecture. . The Aging Process.

E N D
The Aging Eye Dr. Desinee Drakulich
Disclosure Statement • I have no affiliation or get paid by any of the companies who’s products I discussed in this lecture.
The Aging Process • Aging is a continuous, complex, and dynamic process that begins with birth and ends with death. And unless we die in our early years, each of us will grow old and experience the effects of the aging process. • Unfortunately, no reliable measurement exists that allows us to determine the biological age of humans. The most promising, however, are in the realm of genetic and cellular functioning. Two biological phenomena appear related to the aging process: • •Accumulation of waste products in the cells • •Loss of elasticity of the connective body tissue • The human eye undergoes all the same aging changes as the rest of the body.
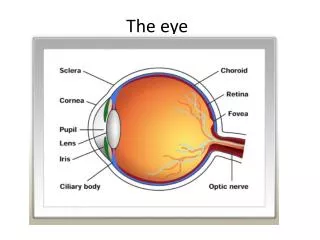
Today we will cover: • The normal and abnormal effects of aging on the eye from the lids to the optic nerve (front to back) • Structures that will be covered: • Eyelids Vitreous • Tear Film Retina • Sclera Optic Nerve • Cornea Eye Muscles • Iris • Angle • Lens
Eyelids • Dermatochalasis- redundant and lax eyelid skin and muscle is known as dermatochalasis. Dermatochalasis is a common finding seen in elderly persons and occasionally in young adults. Gravity, loss of elastic tissue in the skin, and weakening of the connective tissues of the eyelid frequently contribute to this lax and redundant eyelid tissue. These findings are more common in the upper eyelids but can be seen in the lower eyelids as well. • Dermatochalasis can be a functional or cosmetic problem for the patients. When functional, dermatochalasis frequently obstructs the superior visual field. In addition, patients may note ocular irritation, entropion of the upper eyelid, ectropion of the lower eyelid, blepharitis, and dermatitis. When cosmetic, patients note a fullness or heaviness of the upper eyelids, "bags" in the lower eyelids, and wrinkles in the lower eyelids and the lateral canthus.
Ectropion • Ectropion is the turning out of the eyelid (usually the lower eyelid) so that the inner surface is exposed. • Ectropion is usually caused by the aging process and the weakening of the connective tissue of the eyelid, which causes the lid to turn out.
Dermatochalasis • Treatment the treatment of dermatochalasis is surgical (blepharoplasty). The following medical treatments may be appropriate: • •Dermatochalasis patients with blepharitis may benefit from lid hygiene and topical antibiotics. • •Dermatochalasis patients with dermatitis may benefit from topical steroid ointment. • •Dermatochalasis patients with dry eyes should be treated with the appropriate topical lubricant. In addition, placement of temporary collagen punctal plugs, permanent punctal plugs, or punctal cautery may be considered in patients with a history of dry eye or a physical examination consistent with dry eye. These measures may be used preoperatively to further evaluate the patient prior to embarking upon surgery.
Mechanism of MGD • Androgen deficiency, such as occurs during menopause, aging, Sjögren's syndrome, complete androgen insensitivity syndrome and the use of anti-androgen medications, leads to meibomian gland dysfunction, altered lipid profiles in meibomian gland secretions, decreased tear film stability and evaporative dry eye.
Meibomian Gland Dysfunction • The meibomian glands are located in the eyelids. Secretions from these glands comprise the lipid (oily) layer of the tear film which is so crucial in preventing rapid evaporation of the tears. Failure of these glands to produce or secrete oil - due to chronic blockage, thickening of the meibum, etc. will affect the quality and stability of the tear film, which in turn will produce classic dry eye symptoms even in people whose dry eye test results appear normal. • As we age oil viscosity increases and the loss of functioning meibomian glands increases.
Tear Film • The tear film is composed of three layer. • Lipid layer – produced by meibomian glands in the upper and lower eyelids. • Aqueous layer – produced by the lacrimal gland. • Mucin layer – produced by the goblet cells in the conjuctiva.
Meibomian Gland Dysfunction • Treatment: • Warm compresses • Digital massage • Lid hygine • Artificial Tears – Systane, Optive, Thera Tears, Genteal • Topical antibiotics – Azasite • Oral antibiotics – Doxycycline • Topical Steroids – FML, Pred Forte, Lotemax
Lipid Layer • Produced by meibomian glands in the eyelids. • Function is to decrease evaporation rate of aqueous tears and give a smooth blinking surface. • Decreased production secondary to meibomian gland dysfunction and/or damaged meibomian glands.
Aqueous Layer • Usually caused by inflammatory changes associated with autoimmune disorders Sjogrens, SLE and Rheumatoid Disease. • Not necessarily associated with aging. • Produced by the lacrimal gland.
Aqueous Deficiency / Goblet Cell Damage • Inflammation of the lacrimal gland can also increase with age. This inflammation can reduce to quantity of aqueous tears produced. This is most commonly treated with Restasis. • Restasis is a cyclosponin drop use to decrease inflammation and stimulate the lacrimal gland to increase tear production. • Goblet cell damage from sun exposure or autoimmune disorders can decrease mucin production decreasing tear film stability. Often difficult to treat may need surgical mucous membrane grafting.
Aging changes to the Sclera • Thins • Density • Color • Water retention • Uveal Sclera Output decreases • Increase in growths
Normal Aging Changes of the Cornea • Over time, the cornea becomes flatter • Thinner • Slightly less transparent • Its refractive index increases • Descemet's membrane becomes thicker. Increases from 3 u at birth to 10 u in adults as a result of the increased thickness of its posterior non-banded zone. • Occasional peripheral endothelial gutatta, sometimes known as Hassall-Henle bodies, can form with age. • Age-related attrition of corneal endothelial cells results in a loss of about 100,000 cells during the first 50 years of life, from a cell density of about 4,000 cells/mm2 at birth to a density of 2500 - 3000 cells/mm2 in older adults. The average rate of endothelial cell density decrease throughout adult life is approximately 0.6% per year.
Epithelial Layer • It acts as a barrier to protect the cornea, resisting the free flow of fluids from the tears, and prevents bacteria from entering the epithelium and corneal stroma. • Epithelial Layer is made up of 4 types of cells • Surface – squamous cells • Second – prickle cells • Third – wing cells • Fourth – columnar basal cells • Constantly undergoing mitosis.
Bowman’s Layer • a tough layer that protects the corneal stroma, consisting of a similar irregularly arranged collagen fibers
Epithelial Basement Membrane Dystrophy • Corneal map-dot-fingerprint dystrophy is by far the most common corneal dystrophy and is named from the appearance of its characteristic slit lamp findings. Map-dot-fingerprint dystrophy is also known as Cogan’s dystrophy, Cogan microcystic epithelial dystrophy, epithelial basement membrane dystrophy, and anterior basement membrane dystrophy
Stromal Layer • A thick, transparent middle layer, consisting of regularly arranged collagen fibers along with sparsely distributed interconnected keratocytes, which are the cells for general repair and maintenance. • Changes in the morphology of the collagen fibers in the stroma can cause an irregularity to the fibers causes a hazy in the stroma that can effect the clarity of the cornea and visual acuity.
Arcus Senilis • Is a white or gray opaque ring in the corneal margin (peripheral corneal opacity), white ring around the iris. It is quite commonly present in the elderly. It can also appear earlier in life as a result of high cholesterol. • It results from cholesterol deposits in or hyalinosis of the corneal stroma and may be associated with ocular defects or with familial hyperlipidemia.
Descemet’s Membrane • Descemet's membrane is the basement membrane that lies between the stroma, and the endothelial layer of the cornea. It is composed of a different kind of collagen.
Fuch’s Endothelial Dystrophy • Fuchs endothelial dystrophy is characterized by an asymmetrical, bilateral, slowly progressive edema of the cornea in elderly patients. • The root cause of the condition is a slowly progressive formation of guttate lesions between the corneal endothelium and the Descemet membrane.
Guttata • Bumps that form between Descemet’s Membrane and the Endothelial layer. • Signs that the endothelial pumps are not working correctly.
Pupil myosis • The pupil becomes smaller and less responsive to variations in light. • Because the pupil controls the amount of light that reaches the retina, age-related changes to the pupil may affect vision in many ways. First, as the pupil decreases in diameter, seeing well in dim light becomes harder. In addition, the less able the pupil is to adjust to varying light conditions, the less tolerable glare becomes and the more difficult it is to adapt from darkness to bright light or vice versa. This means as you get older, you may need more time to adjust to changing levels of illumination, such as going from bright sunshine into a dimly lit room or restaurant.
Iris Atrophy • A thinning of the iris secondary to loss of pigment and elasticity of the iris.
Floppy Iris Syndrome • A prolapse and constriction of the iris during cataract surgery that can cause serious complications. • Caused by alpha -1- antagonist (a specific drug type). • Major drug of concern is Flomax ( a prostate medication)
Angle Narrowing • Two significant causes: • Cataract formation – cataract enlarges the size of the lens with can decrease the space in the anterior chamber. • Flattening of the cornea secondary to a decrease in collagen fiber elasticity.
Lens • The lens of the eye begins to lose elasticity. • In the same way that losing flexibility in tendons and muscles makes it more difficult for the body to move, losing lens elasticity also makes it harder for the lens to bend in order to focus on closely held objects. This loss of focusing power, or lens accommodation, is known as presbyopia.
Age-Related Cataracts • A cataract is simply an opacification of the crystalline lens of the eye. • There are really three types of age-related cataracts: • Nuclear cataract - which is located in the center of the lens, the nucleus, is most commonly seen as it forms. It is said that the cause of this cataract is due to changes in the protein structure as we age. • Cortical cataract - starts of on the outside of the lens and slowly extends to the center. This cataract is common for the elderly and diabetics. • Posterior Subcapsular cataracts - begins at the back of the lens. People who have a higher risk of developing this form of cataract are: people with diabetes, high farsightedness, retinitis pigmentosa or those taking high doses of steroids.
Vitreous • The vitreous is a thick, transparent substance that fills the center of the eye. It is composed mainly of water and comprises about 2/3 of the eye's volume, giving it form and shape. The viscous properties of the vitreous allow the eye to return to its normal shape if compressed. • In children, the vitreous has a consistency similar to an egg white. With age it gradually thins and becomes more liquid. The vitreous is firmly attached to certain areas of the retina. As the vitreous thins, it separates from the retina, often causing floaters.
Vitreous Syneresis • Floaters are deposits of various size, shape, consistency, refractive index, and motility within the vitreous, which is normally transparent.They may be of embryonic origin or acquired due to degenerative changes of the vitreous or retina.Floaters are visible because of the shadows they cast on the retina or their refraction of the light that passes through them, and can appear alone or together with several others in one's field of vision. They may appear as spots, threads, or fragments of cobwebs, which float slowly before the observer's eyes.
Asteroid Hyalosis • Calcium deposit that form in the vitreous. Patient is usually asymptomatic with little to no vision loss.
Posterior Vitreous Detachment • occurs when the vitreous, a gel-like substance attached to the retina in the back of the eye, shrinks and pulls away from the retina.
PVD • Posterior Vitreous Detachment • Symptoms – flashing light and/or floating spots with little or no vision loss and little or no visual field loss. • Symptoms – patients often describe it as a cobweb or flys in their vision. • What can happen to the eye- generally nothing, however, in rare causes as the vitreous detaches from the retina it can tear or pull the retina off. • Signs of a retinal detachment – increase in flashing lights, increase in floating spots, a decrease in vision and a curtain or vale in the vision.
Aging Changes in the Retina • Photoreceptor and Ganglion Cells • Oxidative stress. Cellular damage caused by reactive oxygen intermediates (ROIs) such as free radicals, peroxides, and single oxygen species. Can also occur from the presence of polyunsaturated fats and continuous exposure to light. • Cell number reduction. Rod cells (periphery) normally reduce by approximately 30% with age, leading to diminished night vision. Number of cone cells (central) normally remains fairly stable. Number of rod cells is approximately 120 million. Number of cone cells is 6.3 to 6.8 million. • Bruch's membrane • Drusen. Accumulation of lipids and photoreceptor cell waste material. Soft drusen can lead to neovascularization. Hard drusen is not necessarily a precursor of macular degeneration. • Choroid • Reduced blood flow. Possibly caused by accumulation of waste and retinal pigment epithelium (RPE) ischemia. Can lead to malnutrition of the photoreceptor cells.
Macular Degeneration • Age-related macular degeneration (AMD) is a chronic condition that causes central vision loss. It affects millions of Americans. In fact, it is a leading cause of blindness in people 60 and older. The older you are, the greater your chance of being affected. • AMD symptoms include blurriness, wavy lines, or a blind spot. • You may also notice visual distortions such as: • • Straight lines or faces appearing wavy • • Doorways seeming crooked • • Objects appearing smaller or farther away • Two forms of Macular Degeneration – Dry and Wet
Risk Factors • Age • Smoking • Light colored eyes • Family History • Poor diet • UV exposure
Vascular System • Hypertension and Hypercholesterol • Vascular narrowing • Cholesterol plaques
Optic Atrophy • Blood pressure and cholesterol problems can cause a stroke in the eye.
Ocular Muscles • Decomposition of ocular muscles can cause diplopia secondary to ocular deviation.
Thank you for your attention • Any questions? • Thank you to the NOA.
References • Kaiser, Friedman, and Pineda. “The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology” Second Edition. 1998 • Onofrey, SkorinJr, and Holdeman. “Ocular Therapeutics Handbook, A Clinical Manual” Second Edition. 1998 • National Health Institute. “ Facts about Macular Degeneration” www.nei.nih.gov • AMDF: American Macular Degeneration Foundationwww.macular.org • National Health Institute. “Facts about Glaucoma” www.ncbi.nlm.nih.gov