Download
1 / 44
520 likes | 1.03k Views
Blood chemistry Hb Structure & Functions. Dr. Vishnu Kumar Awasthi Assistant Professor – In – Charge HLS, Department of Biochemistry. Objectives. Structure of hemoglobin Transport of oxygen by Hb Oxygen dissociation curve (ODC) Factors affecting ODC

E N D
Blood chemistryHb Structure & Functions Dr. Vishnu Kumar Awasthi Assistant Professor – In – Charge HLS, Department of Biochemistry
Objectives • Structure of hemoglobin • Transport of oxygen by Hb • Oxygen dissociation curve (ODC) • Factors affecting ODC • Heme-heme interaction and co-operativity • Effect of pH and pCO2 • The Bohr Effect • The chloride shift • Effect of temperature • Effect of 2,3-BPG • Transport of CO2
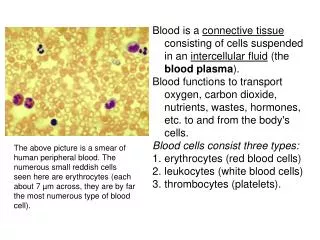
Haemoglobinstructure • Haemoglobin (Hb) is the most abundant porphyrin – containing compound. • It is a tetramer made up of four subunits. • Each subunit contains a heme group and a polypeptide chain.
Haemoglobin structure • Normal level of Hb in blood of males is 14 – 16 g/dl and in females, 13 – 15 g/dl. • Normal adult blood contains 97% HbA, about 2% HbA2 and about 1% HbF.
What is Porphyrin ? N Porphyrin Pyrrole HC HC HC CH HC CH HC C C CH NH N CH HC C C NH HN CH HC C C N C CH HC C CH CH
Heme Heme = Porphyrin + iron
Hemoglobin is a O2 and CO2 transport protein found in the RBCs • Hemoglobin is an oligomeric protein made up of 2 α β dimers, a total of 4 polypeptide chains: α1 β1 α2 β2. • Total Mrof hemoglobin is 64,500. • The α (141 aa) and β (146 aa) subunits have < 50 % identity.
• The 3D- structures of α (141 aa) and β (146 aa) subunits of hemoglobin and the single polypeptide of myoglobin are very similar; all three are members of the globin family. • • Each subunit has a haem-binding pocket
The polypeptide chains are of five types viz. α, β, γ, δ and ε • The α chain is made up of 141 amino acids. • The β , γ, δ and ε chains are made up of 146 amino acid residues each.
Normal adult haemoglobin (HbA) is made up of four haem groups, two α chains and two β chains, and is represented as α2 β2. • A small amount of HbA2 is also found in adults which is α2 δ2. • Foetal haemoglobin (HbF) is α2 γ2 • Embryonic haemoglobin isα2 ε2
The histidine residues linked to iron are present at positions 58 and 87 in α chains and at positions 63 and 92 in other chains. • The bond between iron and the distal histidine residue (His87 or His92) is unstable.
The distal iron-histidine bond is broken when haemoglobin is exposed to high oxygen tension • This results in the formation of an iron-oxygen bond • The binding of oxygen to haemoglobin changes the conformation of haemoglobin
Two conformations have been described, T (taut) and R (relaxed). • Deoxygenated Hb exists in T form which is stabilised by 2,3-bisphosphoglycerate (2,3-BPG) which is formed from 1, 3-BPG (an intermediate in glycolytic pathway) when there is a deficiency of oxygen in the tissues.
T and R states of Hemoglobin • • Hemoglobin exists in two major conformational • states: Relaxed (R ) and Taut or Tense (T) • • R state has a higher affinity for O2. • • In the absence of O2, T state is more stable; when O2 • binds, R state is more stable, so hemoglobin • undergoes a conformational change to the R state. • • The structural change involves readjustment of interactions between subunits
There is a central cavity in the haemoglobin molecule surrounded by the four polypeptide chains. • 2,3-BPG enters this cavity and cross links the two β chains. • When oxygen tension increases, 2,3-BPG is displaced and the T form changes into R form. • During this transition, one pair of α and β subunitsrotates by 15° relative to the other pair.
Each subunit of haemoglobin can bind one oxygen molecule. • Since there are four subunits in a molecule of haemoglobin, one molecule can bind four oxygen molecules.
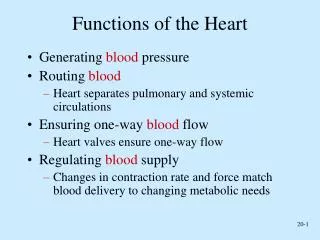
Transport of oxygen by Hb Hb has all the requirements of an ideal respiratory pigment: • It can transport large quantities of oxygen • It has great solubility • It can take up an release oxygen at appropriate partial pressure • It is powerful buffer.
Oxygen dissociation curve • i. The ability of Hb to load and unload oxygen at physiological pO2 is shown by oxygen dissociation curve (ODC)
A Percentage saturation pO2 in mm of Hg
B Percentage saturation pO2 in mm of Hg
C Percentage saturation pO2 in mm of Hg
D Percentage saturation pO2 in mm of Hg
A. Theoretical curve as per mass action. • B. Sigmoid curve, due to heme-heme interaction (hill effect). • C. Further shift to right due to carbon dioxide (Bohr effect) and BPG. This curve represents the pattern under normal conditions. • D. further shift to right when temp is increased to 420C.
ii. At the oxygen tension in the pulmonary alveoli, the Hb is 97% saturated with oxygen. Normal blood with 15 gm/dl of Hb can carry 20 ml of oxygen /dl of blood. • iii.In the tissue capillaries, where the pO2 is only 40 mmHg, theoretically Hb saturation is 75%. Thus under STP conditions, blood can release only 22%.
Factors affecting ODC • 1.Heme-heme interaction and co-operativity:- • A. the sigmoid shape of ODC – due to allosteric effect, or co-operativity. • equilibrium of Hb=O2 Hill equation (A V Hill, nobel prize,1922)
B. Positive co operativity Hb HbO2 HbO4 HbO6 HbO8 Homotropic interaction
c. Each successive addition of O2, increase the affinity of Hb to O2 synergistically. • D. Similarly, binding of 2, 3 – BPG at a site other than the oxygen binding site, lowers the affinity for oxygen (heterotropic interaction).
Alteration of structure Diagrammatic representation of subunit interaction in Hemoglobin
During oxygen uptake, the T form to the R form with disruption of the salt bridges . • The Hb subunits are moved relative to one another. • During oxygenation, the α1 - β2 interface shows movement. • The two subunits slip over each other. • The quaternary structure of oxy Hb is described as R form; and that of de-oxy Hb is T form.
When oxygenation occurs the salt bonds are broken successively. Thus on oxygenation, the Hb molecule can form two similar dimers. (2x alpha)+(2x beta)→2x(alpha-beta) (Deoxy-Hb) (oxy-Hb)
3. The Bohr Effect • The influence of pH and pCO2 to facilitate oxygenation of Hb in the lungs and deoxygenation at the tissues is known as the Bohr effect (1904). • Binding of CO2 forces the release of O2 • When the pCO2 high, CO2 diffuses into the RBCs CO2 + H2O → H2CO3→ H+ + HCO3- Carbonic Anhydrase Iv. When carbonic acid is ionizes, the intracellular pH falls. The affinity of Hb for oxygen is decreased and oxygen is unloaded
O2- HCO3- Cl- 4. The chloride shift • When CO2 is taken up ----HCO3- ↑ CO2 H2O + CO2 Cl shift (in tissues) Carbonic anhydrase H2CO3 HbO2 H+ N N HCO3- HHb +O2 Cl- To cells Chloride enters into RBC
When the blood reaches the lungs, reverse reaction takes place
O2- HCO3- Cl- 4. The chloride shift • When O2 is taken up ---- Air H2O + CO2 CO2 Cl shift (in lungs) Carbonic anhydrase H2CO3 HbO2 H+ N N HCO3- HHb +O2 Cl- Air Chloride comes out of RBC
5. Effect of temperature • p50 = the pO2 at which Hb is half saturated • p50 of normal Hb = 26 mmHg (at 37oC) • Elevation of temp. causes 88 % increase in p50 • ODC shifts to left at low temp. • Under febrile conditions , increased needs of oxygen met by a shift in ODC to right.
6. Effect of 2,3-BPG • Normal 2,3-BPG level=15 ± 1.5 mg/g Hb. • 2,3-BPG == high in children • 2,3-BPG is produced from 1,3-BPG, an intermediate of glycolytic pathway. • 2,3-BPG, preferentially binds to deoxyHb and stabilizes T form • When T form reverts to R, 2, 3-BPG ejected • During oxygenation, BPG released
Transport of CO2 • At rest, about 200 ml of CO2 is produced /minute in tissues. The CO2 is carried by the following 3 ways:- 1. Dissolved form: CO2 + H2O H2CO3 HCO3- + H+
2. Isohydric transport of CO2 • Haldane effect: The H+ ions are buffered by the deoxyhemoglobin. • In tissue • Oxy-Hb is more – (negatively) charged than deoxy-Hb 4. In the Lungs H - Hb + 4O2 Hb (O2)4 + H+
5. The proton released in the RBC combine with HCO3- forming H2CO3 which would dissociate to CO2, that is expelled through pulmonary capillaries. 6. As the HCO3- level inside the erythrocytes falls, more and HCO3- gets into the RBC, and chloride diffuse out.
3. Carriage as carbamino- Hb R-NH2 + CO2 R-NH-COOH 4.Clinical Applications. 1- Hypoxic states,O2 affinity decreased. - ODC shift right. - increased in 2,3-BPG increased in RBC. 2. In anemia, increased oxygen unloading will ensure proper oxygenation of tissues. 3. 2,3-BPG level varies as Hb conc.
4. The Red cell 2,3-BPG level is decreased in acidosis and increased in alkalosis, ODC shift to right. 5. Transfusion of large vol. of stored blood which has a low level of 2,3-BPG can lead sudden hypoxia and a left shifted ODC.