Download
1 / 23
230 likes | 258 Views
Learn to recognize and treat vestibular emergencies in pets. Understand clinical signs, diagnostic testing, and therapeutic interventions for central and peripheral causes. Know when to refer for advanced care.

E N D
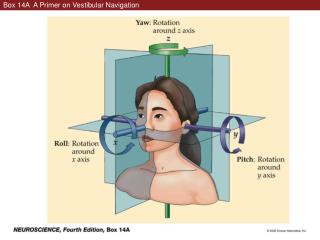
Neurologic Emergencies: vestibular events Todd M. Bishop, DVM, DACVIM (Neurology) Thursday February 6th, 2014
Goals of this mini-lecture • Recognize the clinical signs • Correlate with the neurologic exam • Perform point-of-care diagnostic testing • Provide initial therapeutic intervention(s) • Know when to discuss referral * Making anatomic and differential diagnoses will NOT be emphasized in this talk but the details are in the notes.
What the client sees … • Head tilt • Balance loss; walking as if “drunk” • Jerking eye movements • Eyeball deviation • Nausea, vomiting, drooling • Wide-based stance • Inability to stand • Listing, leaning, falling to one direction • Rolling to one side (“alligator rolling”)
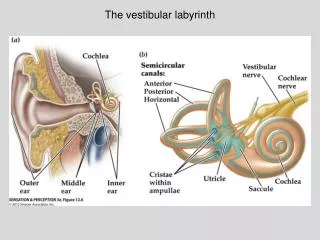
What you should look for … • Mentation change • Cranial nerves abnormalities • Strabismus, nystagmus • Gait and Posture alteration • Head tilt, ataxia • Posturalreactions deficits • Delayed hopping and placing www.rawstory.com
The quick and dirty • When is it in the brain (central vestibular)? • Mentally inappropriate • Vertical nystagmus • Changing direction nystagmus • Right to left • Vertical to horizontal • but NOT horizontal to rotary to the same side! • Postural reaction deficits
Etiologies* PERIPHERAL • Idiopathic • Otitis M/I • Hypothyroidism • Ototoxicity • Trauma • Neoplasia CENTRAL • Metabolic • Malformative • Inflammatory • Infectious • Infarction (vascular) • Neoplastic • Degenerative * Remember this is NOT the emphasis of this lecture!
Diagnostic testing • Primary Care • CBC/Chem/UA/CXR/BP • Thyroid panel • Otoscopic exam • Cytology and culture • Myringotomy • Sedated skull radiographs • Referral • MRI > CT scan • CSF tap
Basic Medical Work-up • CBC/Chem/T4/UA • Thoracic radiographs • A BLOOD PRESSURE
Soapbox ALERT ! • I can not emphasize the importance of the basic medical work-up enough ! • You may find the cause or a complicating disease process !! • This MUST be done before advanced testing can be considered !!! • People … it makes financial sense !!!! • with one exception … same day referral marvimarti.com
Thyroid testing • A simple total T4 will suffice for cats • Dogs need a complete thyroid panel HYPERT4→high BP→stroke→vestibular signs hypoT4→atherosclerosis→stroke→vestibular signs hypoT4→abN metabolism in VIII→vestibular signs
Otoscopic exam http://www.petearclinic.com/images_video.htm
External ear cytology & culture http://leicesterskinvet.com/wp-content/uploads/2010/10/Malassezia-pachydermatis.jpg
Myringotomy (tympanocentesis) http://www.welchallyn.com/apps/products http://glomed.biz/products.php?sub_id=40 http://www.rush.edu/webapps/rml/RMLTestEntryDtl.jsp?id=3264 http://www.neuralstainkit.com/Laboratory_Supplies.php
Sedated skull radiographs Textbook of Veterinary Diagnostic Radiology- Thrall
Empiric therapies * • IV fluids • Antibiotics • Dimenhydrinate (Dramamine) • Meclizine (Bonine, Antivert) • Cerenia • Benzodiazepines • Corticosteroids? * Regardless of etiology!
Intravenous Fluids • Rehydrate after vomiting • Maintain vascular volume (anorexia) • Combat ongoing losses (drooling) • Promote cerebral profusion (especially important in ischemic cerebrovascular disease)
Antibiotic therapy • Common otic flora • Strep, Staph, Malassezia • Base treatment on cytology and culture • Empiric treatment options: • Cephalosporin • Amoxicillin • Fluoroquinolone • Fluconazole
Dimenhydrinate • Antihistaminic (H1), antiemetic and anticholinergic effects • Acetylcholine stimulation of the vestibular and reticular systems may be blocked • 4-8 mg/kg PO SID-TID • 12.5 mg PO SID-TID (cat) • 25–50 mg PO SID-TID (dog) essex1.com
Meclizine • Antihistamine with sedative & antiemetic effects • H1 receptor blocker • 25 mg / dog PO SID x 3-4 days • 12.5 mg / cat insightpharma.com
Cerenia • Maropitant (mar-oh-pit-ent) Citrate • Neurokinin (NK1) Receptor Antagonist • Inhibits Substance P a neurotransmitter involved in vomiting • Acts at the vomiting center to treat motion sickness • 8 mg/kg PO q 24h for up to 2 consecutive days vinoenpaso.at
Benzodiazepines • Diazepam or Midazolam : • 0.5 mg/kg IV bolus • 0.5 mg/kg/hr IV CRI over 24-72 hrs • Sedative effect • Inhibitory neurotransmitter in the vestibular system • Metronidazole toxicosis antidote bipolarblast.wordpress.com
Corticosteroids • Should ideally be employed only after a definitive diagnosis has been made • Can be added if all other empiric therapies are failing and clients not interested in referral • If using empirically consider an anti-inflammatory dose (ie. Prednisone 0.5 mg/kg BID)
When to refer a case? • After a patient is stabilized • Once preliminary testing is done • When there is no response to general supportive care described above • When central disease is suspected