Download
1 / 29
290 likes | 301 Views
This presentation delves into the prognosis of status epilepticus, covering mortality rates, etiology, predictors, and impact on functional outcomes and other disorders. Understand the implications of SE in different populations to better guide treatment and improve patient care.

E N D
DUNE, Paris, December 13 2012Status epilepticus prognosis Andrea O. Rossetti, Service de Neurologie, CHUV, Lausanne, Switzerland
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Why care? « Framing » of clinical setting Should orient treatment resources Might improve SE patients care Prognosis of what ? • Mortality • Functional outcome
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Mortality Short-term: 7%-39% Long-term: 43% at 10 years (RR=3 vs. controls) Logroscino Neurology 2002
EtiologyEpilepsia 1993, DeLorenzo Neurology 1996, Rossetti JNNP 2006 • Acute symptomatic (60%-80%) • Remote symptomatic (10%-20%) • Progressive symptomatic (10%-20%) • Idiopathic (1%-3%) • Up to 50% without previous seizures !
Etiology De Lorenzo Neurology 1996 • CNS infection 36% • AED withdr. 18% • Idiopathic 17% • Amare Epilepsia 2008 Adults • AED withdrawal 34% • Remote sympt. (stroke) 24% • Acute stroke 22% • Metabolic 15% • OH 13% • Anoxia 13% • Idiopathic 3% Children • Infection 52% • Remote symptomatic 39% • AED withdrawal 21%
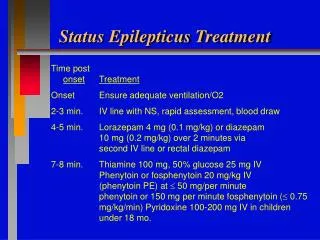
Mortality predictors • EtiologyTowne Epilepsia 1994, Logroscino Epilepsia 1997, Novy Epilepsia 2010 • AgeTowne Epilepsia 1994, Logroscino Epilepsia 1997, Rossetti JNNP 2006 • Consciousness impairmentShneker Neurology 2003, Rossetti JNNP 2006 • Treatment >1hTowne Epilepsia 1994 (but ≠ Logroscino Epilepsia 1997, Rossetti JNNP 2006, Drislane Epilepsia 2009 !) • InfectionsSutter Epilepsia 2012 9
Prognosis : semiology • GC-SE • Depends on systemic complications, etiology • Non-Convulsive SE Thomas Epilepsia 2007 • Absence (also elderly) : excellent (BDZ) • CPSE : usually good, but not always (…etiology!) • In coma (« subtle ») : very poor (ominous etiologies)
Related to De novo SE Encephalitis Severe consciousness impairment Holtkamp JNNP 2005,Novy Epilepsia 2010 Refractory SE (RSE) • Definition • SE resistant to BDZ and 1 AED (20-40% SE)
Prognosis after RSE Novy Epilepsia 2010 • But: reasonable prognosis after prolonged RSE (15%-40%) Cooper Arch Neurol 2009, Bausell Neurology 2011, Drislane Epil Behav 2011 12
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Prognosis in SE : Risk of epilepsy • 3x as after single seizure Hesdorffer Ann Neurol 1998 • higher after RSEHoltkamp JNNP 2005
Prognosis in SE: cognition 2 Adachi Epilepsia 2005 No difference at all between the groups !
Prognosis in SE : Structural damage Tien Radiology 1995 Fernandez-Torre J Neurol 2006 17
Prognosis in SE : Structural damage No MRI sequelae after 1 year in patients with GTC SE (median duration 1h44)Salmenperä Epilepsy Res 2000 CPSE (« limbic ») neuronal damage ?!? Young Arch Neurol 1998, Bauer Epil Behav 2006, Vespa Neurology 2010 vs. Aminoff Arch Neurol1998, Kaplan Neurophysiol Clin 2000, Meierkord Lancet Neurol 2007 Interpretation: GTC SE also leads to systemic changesMeldrum Arch Neurol 1973, Lothman Neurology 1990, therefore more dangerous
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Impact of SE on other disorders Anoxia: SE independent death predictor (RR=6) Rossetti Neurology 2007 • Similar results for: • Post-stroke SE vs. non-SE (RR=2) Knake Epilepsia 2007 • Cryptogenic SE vs. seizures (RR =2) Logroscino Arch Neurol 2008
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Complications of prolonged ICU stay Cereda Neurocrit Care 2009, Cooper Arch Neurol 2009 • Infections • Thrombosis, embolism • ICU myopathy, neuropathy • Ileus • AED side effects • …
Outcome predictors: practical impact Status Epilepticus Severity Score (STESS) Rossetti Neurology 2006, J Neurol 2008
Outcome predictors: practical impact With similar STESS and mortality, lower intubation rate at CHUV (12%) vs. BWH / MGH (36%) Rossetti J Neurol 2008 « Only » 12/29 RSE patients required therapeutic intubation ! Novy Epilepsia 2010 Interpretation: Patients with favorable STESS may not need early intubation
Does SE treatment influence prognosis? Yes !Aranda Epilepsia 2010 !? 36%(USA) vs. 12%(CH) intubated, same prognosisRossetti J Neurol 2008 Hospit. cohort, 225 incident episodesRossetti J Neurol 2012 ICU-based, 144 episodes Kowalski Crit Care Med 2012
Overview Introduction Mortality predictors Functional impact Role of SE in other disorders Practical impact Conclusion
Conclusion 1 Mortality: keep in mindetiology and age RSE: highermortality and more epilepsy
Conclusion 2 Do not over- (norunder-) treat Try to use predictors to orient treatment
Merci ! Luke Fildes, The doctor, 1891, National Gallery, London