Download
1 / 28
290 likes | 312 Views
Fontan Procedure . Ken Jusko, DO. Case. 39 yo female with h/o tricuspid atresia and A. fib. and prior Fontan. No prior studies available for comparison. Scheduled for cath on 3/30/07 and surgery on 4/4/07 for pacer. MR to evaluate Fontan. Fontan Procedure.

E N D
Fontan Procedure Ken Jusko, DO
Case • 39 yo female with h/o tricuspid atresia and A. fib. and prior Fontan. • No prior studies available for comparison. • Scheduled for cath on 3/30/07 and surgery on 4/4/07 for pacer. • MR to evaluate Fontan
Fontan Procedure • Palliative procedure for patients with cyanotic congenital heart disease, in which they have a functionally single ventricle. • Restores an in-series pulmonary to systemic circulation, removing chronic volume load of the systemic ventricle. • Described in 1971 by Dr. Francis Fontan for surgical management of tricuspid atresia.
Congenital Heart Disease that may benefit from a Fontan • Tricuspid Atresia • Pulmonary Atresia • Hypoplastic Left Heart Syndrome • Double Inlet Ventricle • Isomerism
Evolution of the Fontan • Earliest Fontan was a “atriopulomary” connection. (Right atrium or appendage) • Cx: Atrial dilatation, arrhythmia, and thrombosis. • Early 1990’s: Total cavopulmonary anastomosis. A direct end to side anastomosis (Bidirectional Glenn) • More recently the extracardiac conduit was developed excluded the right atrium all together. • Fenestration of the Fontan into the left atrium can be performed in high risk patients, allowing left to right shunting to decompress the Fontan circuit.
Stage 1 • Routinely the Fontan is performed in 2 stages. • 1st stage: Has the goal of reducing the volume load of the single ventricle. • This is accomplished by a Bidirectional Glenn or Hemi-Fontan. • Usually performed at 4 to 8 months or as soon as the pulmonary vasculature has matured sufficiently to allow the superior vena caval blood flow through the lungs without resulting in an undesirably high SVC pressure.
Norwood introduced the Hemi-Fontan as the 1st of a 2 step procedure for obtaining a total cavopulmonary connection.
Stage 2 • Completion of Fontan procedure is usually performed 12-24 months after the hemi-Fontan. • If performing an extracardiac conduit, the procedure may be postponed to allow the patient to grow and is usually undertaken at about 3 yo.
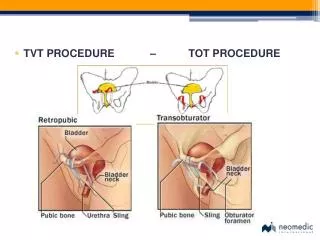
Total Cavo-Pulmonary Connection • Two important features: • Ensure that the opening of the right atrium into the SVC is as large as the IVC opening. • Avoiding suturing of the sulcus terminalis which may cause post operative tachyarrhythmias. • Fenestrate the lateral tunnel to promote decompression of the venous pathway and enhance ventricular filling postoperatively. • These small fenestrations usually close spontaneously.
After bidirectional Glenn the completion of the Fontan procedure can be accomplished using an extracardiac conduit.
Laks advocated the incorporation of an adjustable (snare-controlled) atrial septal defect in hearts with atretic right sided AV connections. • These adjustable ASDs facilitate decompression of the systemic venous system and improved ventricular filling during an early post-op course. • Others have advocated simple fenestration. • After complete recovery the patient can undergo a cardiac catheterization and if satisfactory hemodynamics are observed during a trial occlusion of the fenestration, it may be closed.
Mortality rates have improved with improved modifications. • 1996 report from the Mayo Clinic • 1yr survival 88%, 5yr survival 81% • 1997 (Kaplan Meier) • Estimated 93% 5 yr survival and 91% 10 year survival.
Complications • Arrhythmia • Thrombosis and Stroke • Protein losing enteropathy • Right pulmonary vein compression/obstruction • Fontan Obstruction • Hepatic Dysfunction
References • Balker, C. and Mavroudis, C. Pediatric Cardiac Surgery 3rd Edition. Mosby, Philadlphia (2003). Pgs 496-520. • Braunwald et al. Braunwald’s Heart Disease 7th Edition. Elsevier Saunders, Philadelphia (2005). Pgs. 1516-1523. • Sivasubramanian, M. www.fontanoperation.com. March 28, 2007. • http://www.med.umich.edu/cvc/mchc/parhyp2.htm. University of Michigan Cardiovascular Center. March 28, 2007.