Download
1 / 62
630 likes | 832 Views
The Knee Lecture 11. The Knee Complex. the knee is a large complex joint frequently injured during sport participation the knee is positioned between the two longest bones in the body - the femur and the tibia creating potential for high torque’s

E N D
The Knee Complex • the knee is a large complex joint frequently injured during sport participation • the knee is positioned between the two longest bones in the body - the femur and the tibia creating potential for high torque’s • this factor coupled with poor bony stability makes the knee very susceptible to injury
Tibiofemoral Joint • articulation of the distal femur and proximal tibia form a modified hinge joint • movement in 2 planes - Flex /Ext , lnt /Ext rotation • because of the size and shape of the condyles the tibia can rotate on the femur
this lateral rotation of the tibia on the femur (only a few degrees) provides a locking of the knee or a "screwing-home mechanism" • stability and support provided by menisci and supportive ligaments
Menisci • are fibrocartilage discs that are attached to the tibia by coronary ligaments and joint capsule • they are thicker along the lateral margin and thinner medially • - the medial meniscus is injured more frequently than the lateral meniscus • blood supply only in outer 1/3 of meniscus
Medial Meniscus • 'C' shaped, strongly attached to the tibial surface therefore less mobile • one reason injured more often • also attached to the joint capsule (medially)
Lateral Meniscus • more complete ( almost circle shaped) • loosely attached to tibial surface - less commonly injured
Functions of the Menisci • stability - deepens socket and wedge shaped to prevent A-P motion • -increase surface area of femoral condyles • shock absorption • provide nutrition because it promotes synovial fluid flow and distribution - proprioception function through its innervation
Meniscal Tears • associated with ligaments disruptions, degenerative changes, repetitive stress secondary to chronic ligamentous laxity, isolated or repetitive rotational stresses
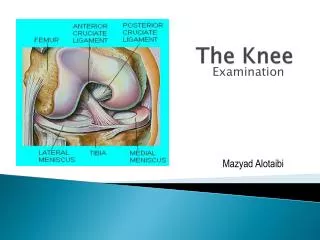
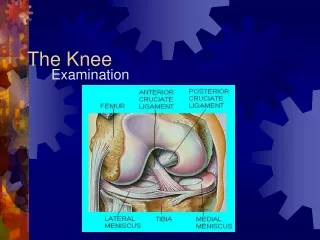
Ligaments of the Knee • the stabilizing role of the ligaments that cross the knee is very significant • two major ligaments are the anterior and posterior cruciates ( called cruciate because they cross each other inside the knee joint) • two other ligaments are the medial and lateral collateral ligaments
Anterior Cruciate Ligament • separated into to bundles according to their functions, ( not really separate) • spiral around one another, insert as one board ligament spiral arrangement plus the broad attachment allow ACL to provide stability through out the full ROM
ACL most common and serious injury to the knee • susceptible to injury with a valgus force, external rotation strong quad contraction of knee hyperextension • ACL is subject to deceleration injuries , internal tibial torque is the most dangerous loading mechanism, particularly when combined with an anterior tibial force
Posterior Cruciate Ligament • not as commonly injured as ACL • stronger and shorter than the ACL • prevents posterior tibial translation and knee hyperextension • common mechanism collision or fall on tibial tuberosity
Medial Collateral Ligament • provide valgus, external rot support (note ACL is also very imp in this function) • basically a thickening of the medial capsule • superficial layer and a deep layer
Lateral Collateral Ligament • cord like structure considered to be extra capsular • less commonly injured b/c of varus mechanism and less debilitating
Dynamic Knee Support • ITB, hamstrings, quads , gracilis , gastroc • the key to injury rehab and prevention
Bursae • Suprapatellar, prepatellar, superficial infrapatellar and deep infrapatellar • i)suprapatellarlargest in the body lies between the femur and the quads tendon of the rectus femoris • ii) prepatellar - located between skin and anterior surface of patella • allowing for movement of then skin over the patella
iii) superficial infrapatellar - located between the skin and the patellar tendon • -inflammation this are due to excessive kneeling referred to as housemaid's knee • iv) deep infrapatellar - located between the tibial tuberosity and the patellar tendon • reduces friction between tendon and bony tuberosity
Patellofemoral Joint • patella articulates with the femur
Patella largest sesamiod bone in the body located within the quads tendon articulates with the femoral condyles patella facets -under surface of patella
1) Contusions and Bursitis • result from a compressive force - a fall , a kick • generally they are locally tender, with pain, swelling and ecchymosis • Bursitis - may be caused by a direct trauma or possibly infection • swelling usually occurs over a 24 hour period • Rx - PIER - protection - may need draining but this may add complications
2) Ligament Injuriesone plane instabilities • i) MCL • pain and swelling usually found along the medial joint line • ii) LCL • pain and swelling are found on the lateral aspect of the knee
MCL injuries • straight lateral forces or valgus causes tension on the MCL
Signs and symptoms • medial knee pain • Swelling • Medial joint laxity • RX - PIER, hinge knee brace for stability , crutches , most MCL injuries are treated non surgically
http://www.youtube.com/watch?v=_fxKCDkOiJs&feature=related • http://www.youtube.com/watch?v=ubP-1WaFeEc&feature=related
LCL injuries • medial forces or varus force produces tension on the LCL • Much rarer injury than MCL
Signs and symptoms • Lateral knee pain • Localized swelling • Lateral joint laxity • RX: PIER, hinge knee brace for stability , crutches , most LCL injuries are treated non surgically
ACL injuries • ACL prevents forward translation of the tibia on the femur, also assists with controlling valgus and varus forces , and helps prevent hyperextension • MOI : damage to the ACL usually results from a cutting or turning maneuver, landing off balance or a sudden deceleration
s/s • Pain , instability , swelling , may often hear or fell a pop in the knee, decreased ROM and function • pain described as being felt deep in the knee or on either side of the patellar tendon • joint effusion is usually bloody and fairly rapid onset
PCL injury • PCl prevents the tibia from moving posterior on the femur • MOI: a direct blow to the anterior tibia ( dashboard injury) , or hyperflexion or hyperextension • s/s • Large tense knee effusion • Discomfort attempting to flex the knee beyond 90 degrees • RX: PIER, crutches , referral to surgeon , however this is not often repairs..
Multidirectional Instabilities – injuries to multiple structures
http://www.youtube.com/watch?v=6evRcL3QMns • http://www.youtube.com/watch?v=uuoj_HFG5Z0&NR=1
First Aid Care ( knee ligaments ) • Apply ice and compression immediately , brace to protect , crutches • If knee unstable , have athlete seek proper medical advice • Most ACL tears are referred to a orthopedic surgeon, due to the continued instability of the knee • Repairs….
3) Meniscal Injuries • compression, tensile and shearing force often cause damage to the mensci • tears may be - longitudinal , bucket handle , horizontal or parrot-beak • medial mensicus is more often damaged • more common in men between the age of 21-40 and women between 11- 20 • joint line pain and general joint effusion, pain with rotations and extreme flexion
individual may experience clicking , popping or grinding • the knee may give way or buckle • the individual may have difficulty doing squats and or duck walking • the meniscal tear may lodge in the joint causing locking • surgery is usually necessary to unlock this condition mensici become stiffer and less resilient with age • RX – PIER – rest and time possibly surgery
First Aid Care • Apply ice and compression immediately ,, crutches • If knee blocked or locked , have athlete seek proper medical advice ASAP • Repairs….
4) Patellofemoral Stress Syndrome • usually caused by weakness in the VMO or lateral retinaculum is too tight • this condition is more commonly found in women due to a higher Q angle • Q angle is the angle between the line of the quads ( RF) and the patellar tendon • a Q-angle of less than 13 and more than 18 may predispose the athlete to PFS
pain may be dull and aching generally in the centre of the knee or on lateral edge of patella • point tenderness usually over lateral edge of patella, often associated with anterior knee pain • crepitus or grinding often present - especially upon compression of the patella • Rx - PIER - NSIADS -taping- VMO strengthening , education