Download
1 / 27
1.41k likes | 4.89k Views
Introduction to Leukemia. Definition Historic Perspective Etiology and Risk Factors Incidence Classification Comparison of Acute and Chronic Leukemia. Leukemia Definition

E N D
Introduction to Leukemia • Definition • Historic Perspective • Etiology and Risk Factors • Incidence • Classification • Comparison of Acute and Chronic Leukemia
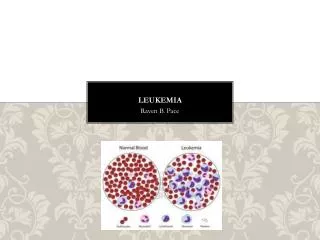
Leukemia Definition Leukemia is a malignant disease of hematopoietic tissue characterized by the accumulation abnormal white cells (neoplastic or leukemic) in the bone marrow leading to bone marrow failure, a raised circulating white cell count (leukocytosis) and infiltrate organs (e.g liver, spleen, lymph nodes, brain)
Leukemia • Historic Perspective • 1945 • The initial description of leukemia as a clinical entity was made by Bennett in Scotland and in Germany.
Leukemia • Etiology and Risk Factors • The etiology of leukemia is unknown. • Oncogenes mutation and tumor suppressor gene alteration. • Host factors. • Environmental factors
Oncogene mutation Tumor suppressor gene Chromosomal abnormality Gene rearrangement Stem Cell ? ? Myeloid series Lymphoid series ? ? Leukemia
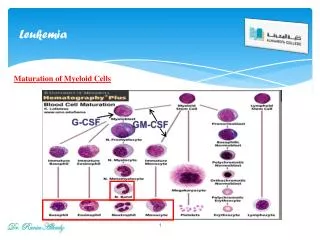
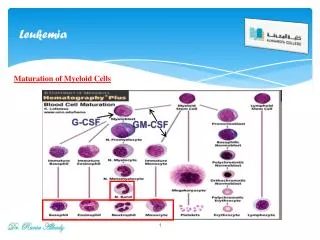
The Role of Oncogenes in Haemopoietic Malignancy • Cellular proto-oncogenes are highly conserved constituents of the normal human genome. • They encode proteins, which act as growth factors, growth factor receptors, signal tranducers or controllers of nuclear function. • In short, proto-oncogen products play a major role in the control of cellular growth, differentiation and division within the body. It is hardly surprising, then, that disruption of proto-oncogen function can lead to malignant transformation.
Oncogene Activation • Four types of chromosomal aberration, which can lead to oncogene activation, commonly, are found in haemopoietic malignancies: • Translocations and inversions. • Deletions and numerical changes. • Point mutations. • Gene amplification.
Host Factors • Congenital chromosomal abnormalities • Increased frequency in patients with congenital disorders that have tendency for chromosomal abnormality. • Such as : Bloom’s syndrome, Fanconi anemia, Down’s and Klinefelter’s syndromes. • 18-20 fold increase incidence of AL is seen in children with Down’s Syndrome.
Immunodeficiency • An unusually high incidence of lymphoid leukemia and lymphoma has been described in patients with hereditary immunodeficiency states (ataxia-telangiectasia and sex-linked agamaglobulinemia). • Usually related to T and B-lymphocyte gene rearrangement.
Chronic bone marrow dysfunction • Patients with CBMD syndromes have an increased risk of acute leukemic transformation. • Examples include the myelodypalstic syndromes, myeloproliferative disorders, aplastic anemia and PNH
Environmental factors Ionizing radiation • Leukemia is associated with exposure to ionizing radiation such as nuclear weapons in Hiroshima and Nagasaki. • Both acute and chronic forms of leukemia including AML, ALL and CML were associated.
Drugs • A variety of drugs have been associated with the development of leukemic transformation • Examples: Benzene, Chloramphenecol, Phenylbutazone and Cytotoxic alkylating chemotherapeutic agents.
Cytotoxic alkylating chemotherapeutic agents • Alkylating agents are strongly electrophilic molecules, which bind to nucleophilic sites on DNA. • They are capable of alkylating the nitrogen and oxygen molecules of all four bases. • This result in inappropriate base pairing, the introduction of strand breaks complex rearrangements and the deletion of parts or all of the chromosomes.
Comparison between de novo &therapy-induced ANLL • At least 90% of therapy induced ANLL cases have cytogenetic abnormalities. The most common findings are monosomy 5, 5q-, monsomy and 7q-. Less than 60% of de novo cases bear cytogenetic abnormalities and chromosomes 5 and 7 are involved less commonly. • More than two thirds of cases of therapy-induced ANLL are preceded by a preleukaemic phase, which is marked by severe dysplastic changes and ineffective haemopoiesis. A preleukaemic phase occurs in less than one quarter of de novo cases. • Therapy-induced ANLL typically is refractory to treatment: the mean survival time from diagnosis is 4 months compared to 20 months in de novo.
Chemicals • Benzene. • Cigarette smokers • Agricultural workers. • Rubber industry workers • Children of the nuclear industry workers • Anesthetists
Viruses • The human T-cell leukemia-lymphoma virus-I (HTLV-I) has been implicated as a causative agent of adult T-Cell leukemia-lymphoma. • Another related virus HTLV-II has been isolated from patients with atypical hairy cell leukemia (CLL) • The Epstein’s Barr virus has been linked to Burkitt’s lymphoma.
Incidence • Overall incidence of leukaemia worldwide 8-10 new cases per 100,000 individuals annually. • About 50% acute and 50% chronic • Leukemia strike more in adult than children (10:1) and has slightly increase incidence in males than females (1-2:1)
Incidence • Acute leukaemia occurs at all ages, but ALL is more common in children and AML is more common in adults. • 75% of childhood leukaemia are classified as ALL, whereas nearly 80% of AMLs occur in adults. • Chronic leukaemia is generally considered as a disease of adults. • CLL is extremely rare in children and is unusual before the age of 40. • CML may be seen at any age, but its peak incidence is between 30 and 50 years of age; the disease is rare in children.
Classification of leukemia Main classification Acute leukemia Chronic leukemia FAB Lymphoid Myeloid Myeloid Lymphoid AML M0 M1 M2 M3 M4 M5 M6 M7 ALL L1 L2 L3 CLL PLL HCL CML
Classification of leukemia • The acute leukemia's. • The chronic leukemia's. • The myelodysplastic syndromes. • The non-leukaemic myeloproliferative disorders. • The non-leukaemic lymphoproliferative disorders.
The Acute Leukemia's • Acute leukaemias are characterized by uncontrolled proliferation of poorly differentiated cells (blasts). The acute leukemias are divided on the basis of the predominant haemopoietic lineage involved into: • Acute lymphoblastic leukaemia (ALL). • Acute non-lymphoblastic leukaemia (ANLL).
Main Classification FAB classification Acute Myeloid leukemia Acute non-Myeloid leukemia ALL L1 L2 L3 AML M0 M1 M2 M3 M4 M5 M6 M7
The Chronic leukaemias • Chronic leukaemias differ from acute leukaemias in that the predominant cell type shows some characteristics of maturity. • Chronic lymphocytic leukaemia (CLL). • Prolymphocytic leukaemia (PLL). • Hairy cell leukaemia (HCL). • Chronic myloid leukaemia (CML).
The Mylodysplastic Syndromes • The mylodysplastic syndromes can be thought of as a preleukaemic condition. They are classified according to the FAB criteria into: • Refractory anaemia (RA). • Refractory anaemia with sidroblasts (RAS). • Refractory anaemia with excess of blasts (RAEB). • Refractory anaemia with excess blasts in transformation (RAEB-t). • Chronic myelomonocytic leukaemia (CMML).
The non-leukaemic myeloproliferative disorders • These are three different non-leukaemic myeloproliferative disorders: • Primary proliferative polycythaemia (PPP). • Primary thrombocythaemia (ET). • Myelofibrosis (MF).
The non-leukaemic lymphoproliferative disorders The diverse group of conditions includes: • Multiple myeloma (MM) and related plasma cell disorders. • Hodgkin's disease (HD). • Non-Hodgkin's lymphomas (NHL).