Download

1 / 22
220 likes | 330 Views
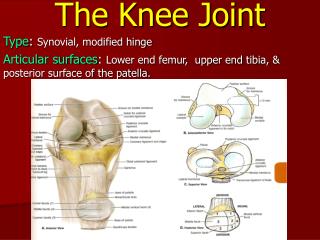
THE KNEE JOINT. CARE & PREVENTION OF ATHLETIC INJURIES MS. HERRERA. FACTS. A.K.A “TIBIOFEMORAL JOINT” A hinge joint ROM: flexion and extension Unstable laterally and medially. Anatomy. Bones: Femur, tibia, fibula, and patella Muscles: Biceps femoris, semitendonosis, and semimembranosus

E N D
THE KNEE JOINT • CARE & PREVENTION OF ATHLETIC INJURIES • MS. HERRERA
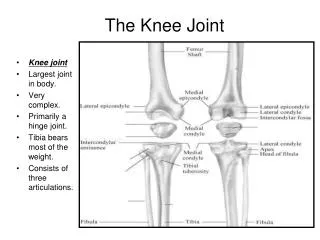
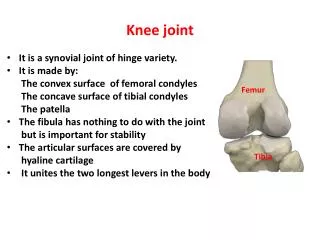
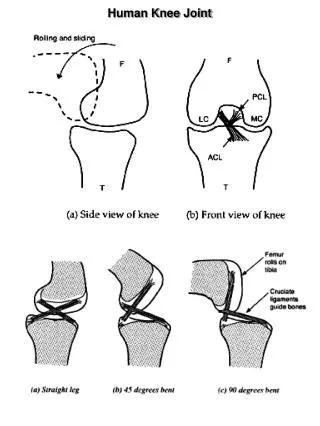
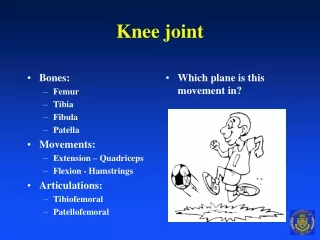
FACTS • A.K.A “TIBIOFEMORAL JOINT” • A hinge joint • ROM: flexion and extension • Unstable laterally and medially
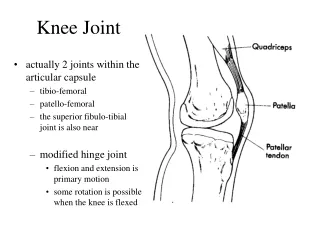
Anatomy • Bones: • Femur, tibia, fibula, and patella • Muscles: • Biceps femoris, semitendonosis, and semimembranosus • Rectus femoris, vastus medialis, vastus lateralis, vastus intermedius • Sartorius (longest muscle in body) and gastrocnemius
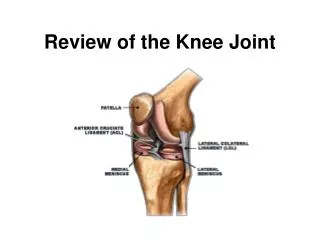
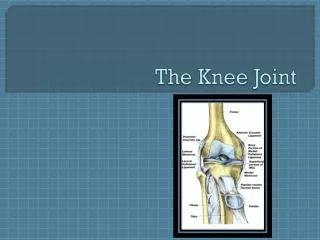
Anatomy Cont’d • Mensicus (you have 2) • Medial mensicus (C-Shaped) • Lateral mensicus (O-shaped) • Made of???? • Ligaments (purpose of each?) • Anterior cruciate ligament • Posterior cruciate ligament • Medial collateral ligament • Lateral collateral ligament
Anatomy Cont’d • Bursae • As many as 2 dozen in the knee • Nerve Supply • Sciatic • tibial • Femoral
Medial Collateral Ligament Sprain (MCL) • MOI: direct blow from lateral side creating excessive valgus stress • Excessive knee twist
MCL Sprain Cont’d • Management • Conservative tx usually • Ice, e-stim, ultrasound, rehabilitation • Surgery is indicated if MCL is sprained along with the ACL or PCL • Categorized into 3 grades • Signs & Symptoms (depends on grade) • Ligament fibers torn/stretched • Pain, swelling (mild-severe) • TTP over MCL and attachment sites • Loss of ROM, joint stiffness, weak • + valgus stress test
Lateral Collateral Ligament Sprain • MOI: Blow to the medial side of the knee causing a varus force • Signs & Symptoms: • Pain, TTP over LCL, swelling • Laxity with varus testing • Management: • Same as MCL
Anterior Cruciate Ligament Sprain (ACL) • Prevents ant. movement of tibia • MOI: valgus force with tibia in external rotation • Noncontact tears more common in females • Why? Several reasons • Signs & Symptoms • Loud pop • Pain, laxity, immediate swelling, and hemoarthrosis (?)
ACL Cont’d • Management: • Not repairing the ACL can lead to joint degeneration. (examples?) • Should be repaired with surgery cause if not it leads to knee instability • Before surgery rehab is usually given to strengthen quadriceps. Why? • Surgery can be allo- or autoGRAFT • difference?
Posterior Cruciate LigamentSprain • Purpose: To prevent posterior translation of the tibia. • MOI: Falling directly on a bent knee • Signs & Symptoms: • Loud “pop” in back of knee • pain, swelling, tenderness over posterior knee, laxity
PCL Cont’d • Management: • Conservative: Rehabilitation-some positive outcomes have been reported. • Surgery to repair torn ligament.
Mensicus Tears • Medial mensicus is MORE commonly injured than lateral mensicus. • Why? Lat. mensicus is more mobile • MOI: Twisting force while foot is planted, cutting motion when running, tears that occur overtime due to high stress (i.e. running)
Mensicus Tears Cont’d • Signs & Symptoms: • Swelling • Locking, clicking • Pain when squatting • Giving way • Management: • Conservative if person is not an athlete or tear is in a vascular zone • Surgery: Indicated for high activity individuals • Can be repaired or resected depending on case
Joint/Muscle Contusions • A.K.A. “Charley Horse” • MOI: Direct blow to the thigh • Signs & Symptoms: • swelling and severe pain • Loss of ROM and strength • Management: • Rest, ice, light stretch • Complete ROM exercises • Apply pad for protection upon RTP • Complications: Myositis ossificans
Patellar Dislocations/Subluxations • MOI: planting leg, slowing down, and cutting suddenly (most common MOI) • Signs & Symptoms: • Obvious deformity, severe pain, swelling, complete loss of knee function
Patellar Dislocations/Subluxations Cont’d • Management: • Keep athlete still and activate EMS • Splint and transfer to ER • Reduce dislocation • Crutches NWB for 4 weeks + • Rehabilitation with focus on quad strengthening
Chondromalacia Patella • Wearing away of articular cartilage on the posterior patella • MOI: Most common abnormal patellar tracking • Causes? • Signs & Symptoms: • Pain, swelling, crepitus • Pain with running, walking, stairs, squatting
Osgood-Schlatter Disease • Pain in patellar tendon where it attaches on the tibial tubercle. • Occurs in adolescents • Athlete may experience multiple avulsions and in severe cases COMPLETE avulsion. • Signs & Symptoms: • Severe pain when kneeling, running, jumping • Inflammation • Enlarged tibial tubercle • Management: Rest, ice before and after activity, strengthening of quads and hamstrings
Patellar Tendinitis A.K.A. Jumper’s Knee • Extreme tension/overuse of the quads. • Places stress on patellar tendon • Signs & Symptoms: • Pain and TTP inferior to the patella • 3 stages of severity • Management: • Nsaids • Rest, Ice, Modalities • Rehab • Cross friction massage
Prentice, William E. Arnheim’s principles of athletic training 12th ed. McGraw-Hill, New York Ny, 2006.