Download
1 / 37
390 likes | 422 Views
DEVELOPMENT OF ATRIA & VENTRICLES. Dr. Mujahid Khan. Fate of Heart Tubes. The tubular heart elongates and develops alternate dilations and constrictions: Truncus Arteriosus Bulbus Cordis Ventricle Atrium Sinus venosus. Partitioning of Heart.

E N D
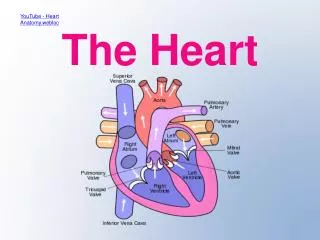
DEVELOPMENT OF ATRIA & VENTRICLES Dr. Mujahid Khan
Fate of Heart Tubes • The tubular heart elongates and develops alternate dilations and constrictions: • Truncus Arteriosus • Bulbus Cordis • Ventricle • Atrium • Sinus venosus
Partitioning of Heart • Partitioning of the atrioventricular canal, primordial atrium, and primordial ventricle begins around 4th week • Completed by the end of the 5th week
Partitioning of Atrioventricular Canal • Toward the end of the 4th week • Endocardial cushions form on the dorsal and ventral walls of the AV canal • The AV endocardial cushions approach each other and fuse • Dividing the AV canal into right & left canals • These canals partially separate the primordial atrium from the ventricle • Endocardial cushion works as AV valves
Endocardial Cushion • It develops from a specialized extracellular matrix (ECM) or cardiac jelly • The transformed endocardial cushions contribute to the formation of the valves and membranous septa of the heart
Partitioning of Primordial Atrium • Beginning at the end of the 4th week • Is divided into right & left atria by the formation and subsequent modification and fusion of two septa: • Septum primum • Septum secondum
Septum Primum • It’s a thin crescent shaped membrane • Grows from the roof of the primordial atrium towards the fusing endocardial cushions • Dividing the common atrium into left & right halves
Foramen Primum • A large opening forms in the growing septum primum between its crescentic free edge and the endocardial cushion • It serves as the shunt, enabling oxygenated blood to pass from right to the left atrium • Becomes progressively smaller and disappears as the septum primum fuses with the fused endocardial cushions to form a primordial AV septum
Foramen Secondum • Perforation appears in the central part of the septum primum before the foramen primum disappears • Perforation coalesce to form another opening, the foramen secondum • Concurrently, the free edge of the septum primum fuses with the left side of the fused endocardial cushions • It ensures a continuous flow of oxygenated blood from right to the left atrium
Septum Secondum • A crescentic muscular membrane • Grows from ventrocranial wall of atrium • Immediately to the right of the septum primum • It is thick and grows during 5th & 6th weeks • Gradually overlaps the foramen secondum in the septum primum
Septum Secondum • It forms an incomplete partition between the atria • Consequently an oval foramen forms • Cranial part of the septum primum ( attached to the roof of left atrium) disappears gradually • Remaining part of septum primum (attached to endocardial cushion) forms a flap like valve of oval foramen
Oval Foramen • Before birth it allows most of the oxygenated blood entering the right atrium from IVC to pass into the left atrium • Prevents the blood flow in opposite direction • After birth it normally closes and the valve of the oval foramen fuses with septum primum • The interatrial septum becomes a complete partition between the atria
Oval Fossa • An oval depression in the lower part of the interatrial septum of the right atrium known as oval fossa • It’s a vestige of the oval foramen
Partitioning of Primordial Ventricle • Division of primordial ventricle is first indicated by a median muscular ridge, the primordial interventricular septum • Is a thick crescentic fold has a concave free edge • Initially most of its height results from dilation of the ventricles on each side of the IV septum
Partitioning of Primordial Ventricle • Medial walls of the enlarging ventricles approach each other and fuse to form the primordium of the muscular part of the IV septum • Active proliferation of myoblasts in the septum increase its size • Until the 7th week there is a crescent shaped interventricular foramen between the free edge of IV septum and the fused endocardial cushion
Interventricular Foramen • The IV foramen permits communication between the right and the left ventricles • It usually closes by the end of the 7th week as the bulbar ridges fuse with the endocardial cushion
Closure of IV Foramen • Formation of the membranous part of the IV septum result from the fusion of tissues from 3 sources: • The right bulbar ridge • The left bulbar ridge • The endocardial cushion
Interventricular Septum • The membranous part of the IV septum is derived from an extension of tissue from the right side of the endocardial cushion to the muscular part of the IV septum • This tissue merges with the aorticopulmonary septum and thick muscular part of the IV septum
Interventricular Septum • After closure of the IV foramen and formation of the membranous part of the IV septum, the pulmonary trunk is in communication with the right ventricle and the aorta with the left ventricle
Trabeculae Carnae • Cavitation of the ventricular walls forms a sponge-work of muscular bundles called trabeculae carnae • Some of these bundles become the papillary muscles and tendinous cords • The tendinous cords run from the papillary muscles to the atrioventricular valves
Tetralogy of Fallot Classic group of four cardiac defects: • Pulmonary stenosis • Ventricular septal defect • Dextroposition of aorta • Right ventricular hypertrophy