Download
1 / 37
370 likes | 533 Views
Quality Improvement In the Carolinas. Leonard Feld, MD, PhD. MMM, FAAP Department of Pediatrics Levine Children’s Hospital Carolinas Medical Center Charlotte, NC. Today’s Objectives. Discuss the Process of Quality

E N D
Quality Improvement In the Carolinas Leonard Feld, MD, PhD. MMM, FAAP Department of Pediatrics Levine Children’s Hospital Carolinas Medical Center Charlotte, NC
Today’s Objectives • Discuss the Process of Quality • Discuss specifics related to Levine Children’s Hospital and the Department of Pediatrics
What is Quality? • The answer is quite simple: “It depends!” • It depends on who is answering the question and what is important to them. • It depends on who is defining quality and how they measure it. • It depends on the theories you accept to guide your quality journey!
The Approach to Quality • Organizational commitment to quality • Focus on the customer • Fix systems, not people • Foster teamwork and group problem solving • Base improvement decisions on data versus intuition • Continuously improve • No quick fixes
Key Elements of System Change • Will to do what it takes to change to a new system • Ideas on which to base the design of the new system • Execution of the changes to system
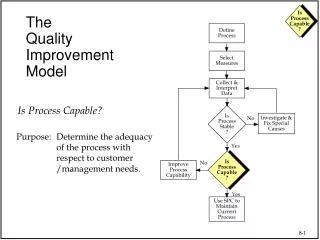
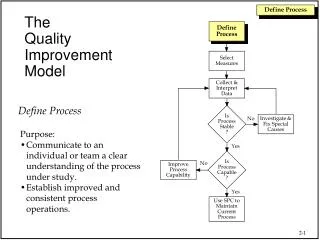
Fundamental Questions for Improvement • What are we trying to accomplish? • How will we know that a change is an improvement? • What changes can we make that will result in an improvement?
Model for Improvement What are we trying to accomplish? • Aim • Measures • Ideas/Change Concepts How will we know that changes are an improvement? What changes can we make that will result in an improvement? The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. G. Langley, K. Nolan, T. Nolan, C. Norman, L. Provost. Jossey-Bass Publishers., San Francisco, 1996.
AIM: What are we trying to accomplish? MEASURES: How will we know that changes are an improvement? IDEAS: What changes can we make that will result in an improvement? Model for Improvement
Importance of Aim Statement • Captures early decisions • Alignment of team • Communication with others • Touchstone throughout project • Key to success
What is an Aim Statement? Aim: A written statement of the accomplishments expected from improvement effort Key components: • A general description of aim - should answer, “what are we trying to accomplish?” • Rationale/importance • Some guidance for carrying out the work • Specify target population and time period • Measurable goals
Goals Should Be: • Measurable • Numeric • Preferably absolute rather than relative • A stretch, not business as usual • Achievable, not impossible
AIM: What are we trying to accomplish? MEASURES: How will we know that changes are an improvement? IDEAS: What changes can we make that will result in an improvement? Model for Improvement
How will we know if a change is an improvement? “All improvement is change, but not all change is an improvement.”
Balancing Measures • Are we improving parts of our system at the expense of others? • Usually not one of goals • Great source is to listen to skeptics… “Yes, but…”
Using Measures: Annotated Run Charts Clinician education Reduced appt delays Practice wide guidelines Reminder system The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. G. Langley, K. Nolan, T. Nolan, C. Norman, L. Provost. Jossey-Bass Publishers., San Francisco, 1996.
AIM: What are we trying to accomplish? MEASURES: How will we know that change is an improvement? IDEAS: What changes can we make that will result in an improvement? Model for Improvement
“Change Concepts” • A general approach to change (e.g., Reduce backlog) • Purpose: to help teams generate specific changes to improve • “Change concepts” come from evidence and models that have been shown to work elsewhere • Feasible and effective in other settings (good ideas) • But need adaptation to specific setting (PDSAs)
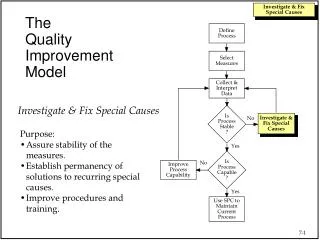
The PDSA Cycle Act Plan • Objective • Questions and predictions • Plan to carry out the cycle (who, what, where, when) • What changes are to be made? • Next cycle? Study Do • Complete the analysis of the data • Compare data to predictions • Summarize what • was learned • Carry out the plan • Document problems and unexpected • observations The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. G. Langley, K. Nolan, T. Nolan, C. Norman, L. Provost. Jossey-Bass Publishers., San Francisco, 1996.
Key Points for PDSA Cycles • Do initial cycles on smallest scale possible • Think baby steps…a “cycle of one” usually best • “Failed” cycles are good learning opportunities when small • Learning from “failed” tests. Ask: • Was test conducted well? • Does the change tested need modification in our setting? • Were measures sufficient to detect improvement? • Was prediction/theory wrong?
Key References • The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. G. Langley, K. Nolan, T. Nolan, C. Norman, L. Provost. Jossey-Bass Publishers., San Francisco, 1996. ( A MUST READ) • http://www.apiweb.org/associates.htm (Provost) • “Eleven Worthy Aims for Clinical Leadership of Health System Reform,” Don M. Berwick, JAMA, September 14, 1994, Vol. 272, #10, p. 797-802.
CAPE History • The Center for Advancing Pediatric Excellence (CAPE) at Levine Children’s Hospital (LCH) developed as the Department of Pediatrics embraced an industry shift toward providing better patient care and QI education. • Leadership in the LCH Department of Pediatrics determined that long-term success of QI initiatives depended on the development of an infrastructure to support ongoing improvement efforts. Residents needed dedicated resources to fully implement QI practice. CAPE resulted from this vision. • Began staffing and operations in the spring of 2009 • Curriculum launch in July 2009, followed by immediate application
Education Innovation: The CAPE Program Initially funded by a Duke Endowment grant, CAPE’s experiential program is unique. It provides intensive, one-on-one QI coaching to each resident within a 3-year, progressive curriculum. CAPE features innovative, multi-faceted, individualized support: • QI Coach • Data Analyst • QI Faculty Mentor • CAPE director, co-director, and other staff Residents join and initiate real QI projects in LCH and associated clinics. Each project funnels into the overall system goals and priorities.
Quality – LCH and CAPELCH Quality Goals and Faculty/Resident Projects Update Noonan, Courtlandt, Doyle, Mabus, Walsh Koricke, and the entire faculty, nurses, residents and professional staff. LCH Quality Goals – Healthcare Acquired Conditions, Appropriate Care Measures, LOS, ED Efficiency Numerous QI projects throughout LCH are advancing with CAPE’s support ; 63 faculty; 29 resident projects Health Literacy Open Access and Office Efficiency Primary care provider communication tool (RHICU) Improve Care NOW (GI) Discharge Prescription Project Reduce CRBSI and VAPs Improve surveillance of chronic GVHD Time from Arrival to Antibiotics Improve Immunizations rate in HIV infected children Standardization processes in the Dialysis Unit CAPE continues to participate in QI education activities
Unique features • Utilizes a multi-faceted approach to teach QI • Didactic lectures • Self-instruction via reading and online modules • Experiential learning through actual projects • Reflective practice • One-on-one coaching • Faculty mentoring • Data management coaching • Employs a progressive 3-year curriculum • Provides a dedicated staff to guide QI endeavors including a QI Coach and support from a Data Analyst
Curriculum • PGY-1 Introduction to the Model for Improvement • Complete pre-assessment QI knowledge survey, Mandatory QI readings • Mandatory IHI online modules, Participation in QI didactic lectures • Personal Improvement Project (PIP), Short Ambulatory QI Project • PGY-2 Experiential learning within a QI team • Mandatory QI readings, Mandatory IHI online modules • Participation in QI didactic lectures, Identify a Faculty QI Mentor • Joins an existing multi-disciplinary QI project, or starts own project
Curriculum • PGY-3 Building leadership and sustainability • Mandatory QI readings and IHI online modules • Participation in QI didactic lectures • Work with Faculty QI Mentor • Functions as a Physician Champion of a multi-disciplinary QI project • Present QI project to broad LCH audience, including Department of Pediatrics faculty • Plans for sustainability of project • Complete post-assessment QI knowledge survey
Quality - Infection Free Days Catheter associated blood stream infections and ventilator associated infection. ICU Pediatric Hematology & Oncology NICU
Children’s Asthma Care Core Measure: Appropriate Care Score This project focuses on the care of inpatients with asthma, the delivery of beta-agonists, corticosteroids, and discharge with a home maintenance plan of care. The Appropriate Care Score reflects the percent of patients who received all required elements.
CHIPS Geography Project Optimizing care teams, ensuring continuity, and effective transitions have been shown to produce improved health outcomes. Co-location of healthcare providers in a specific geographic location is a strategy that can lead to improved continuity, transitions of care, and care teams. LCH CHIPS teams will improve patient’s quality of stay at LCH by implementing geographically located teams. CHIPS physicians will be able to work more closely with a smaller number of nurses, therapists, and consultants, and be in close proximity to our patients throughout the day and night.
Myers Park Pediatric ClinicObesity QI Project The goal of this project is to impact childhood obesity among MP pediatric patients through prevention, monitoring, and management. Identification of patients who are overweight and obese using BMI measurement is essential in managing the pediatric population. The initial phase of this project is development of tools for identification and management of overweight and obese children. Subsequent phases will include evaluation of the presence of documentation of overweight and obesity in the medical record and evidence of provider counseling.
Myers Park Pediatrics Health Literacy QI Project A key strategy to ensuring patient understanding is the use of Teach Back. A pediatric resident is currently spreading her clinic-based Teach Back project to other residents. There is concern that use of Teach Back will increase the length of visits. This project demonstrates a shorter visit length attributed to improved communication and improved patient understanding.
Expedited Partner Treatment for Sexually Transmitted Infections Educate 100% of providers at THC and CMC ED on topic of EPT, including treatment algorithms and prescription instructions Educate 100% of index patients about partner treatment options Increase the percent of patients who are offered EPT by 75% Increase the percent of patients who accept EPT by 75% Notify 100% of positive GC/C cases at THC and CMC ED
The Future of QI at LCH LCH and Dept of Peds is committed to broadening the QI program QI expansion will allow LCH and the Dept of Peds to significantly alter care for children in our own community, and at hospitals across the country. • Additional QI capacity will help our providers gain control over some of the most pervasive diseases plaguing our patients, e.g. asthma and obesity. • QI work will help our hospital reach unprecedented success in care measures like infection prevention and mortality rates. • As the nation addresses healthcare issues, CMC and LCH will need to rely heavily on QI to remain at the forefront of healthcare excellence.
Bottom line on Quality Accelerate cross learning and spread adoption Design systems to foster collaborative networks to learn Frontline leadership drives design and sets measureable QI participation and expectations Avoid stagnation Take population based improvements to the next level Let’s get interested in doing better all the time and achieve sustainability
We Learn – We teach Thank you to our team Laura Noonan, MD Cheryl Courtlandt, MD Sarah Mabus Maureen Walsh Koricke, RN Leslie Doyle, RN Entire LCH and Peds Team