Download
1 / 7
70 likes | 141 Views
Using patient navigation to facilitate utilization of available community resources in patients with or at risk for type 2 diabetes. Overview of R eferral Process to Patient Navigators.

E N D
Using patient navigation to facilitate utilization of available community resources in patients with or at risk for type 2 diabetes
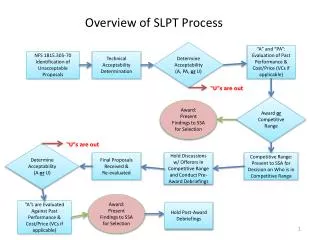
Overview of Referral Process to Patient Navigators • Patients with type 2 diabetes or at risk for diabetes may benefit from services provided by community-based organizations (CBO). • Primary care physicians (PCP) are well positioned to identify individuals who could benefit. • PCPs cannot easily maintain up to date information on CBO. • Patient navigators (PN) maintain data resources and use motivational interviewing approaches to link patients to suitable programs.
Patient Navigators: Start-Up • Compile a list of community resources for patients with diabetes and at risk for diabetes. The Community Action Team can help to populate a list of resources. • Learn, improve, and use a patient tracking data mechanism. • Get involved in project orientation for participating practices and CBOs. • Establish a two-way data transfer for referral and tracking between the PN, CBO and practices.
Patient Navigators: Ongoing • Provide patient navigation services for referred individuals according to the outlined plan. • Provide feedback to participating practices, patients, and CBO. • Maintain and update patient tracking information (including notes of calls, number of phone calls including unsuccessful attempts and time spent on each call/communication). • Provide regular (e.g., quarterly) reports on patient navigation to the project team.
Navigators’ Actions (step-by-step): • Upload patient information and referral forms into the patient data tracker. • Contact the patient. • Explain the program and process to the patient. • Use a scripted paragraph explaining the program protocol and expectation. • Interview the patient using a series of open ended questions that, while still falling under the practice of motivational interviewing, would also provide a uniform approach. • On a scale of 1-10 how satisfied are you with your level of diabetes management? • What would it take to move you from a 2 to a 7 ? (for example) Answers may include meal plan, exercise or access to education or medications. • May I suggest a community resource? • Direct the patient to a community resource. • Notify the community resource of the referral. • Update the referring practice. • Follow up with the patient in 1-3 weeks (notify the practice of patient status). • Note all correspondence.