Download
1 / 35
430 likes | 1.04k Views
Shannon Chan Prince of Wales Hospital. Rectal Carcinoid Current Management and Evidence. Case Scenario . F/47 Ms Ying Good past health Screening colonoscopy by private: 1.5cm rectal polyp at 5cm from anal verge Polyp base elevated with NS and snared Path: Carcinoid, Margin involved.

E N D
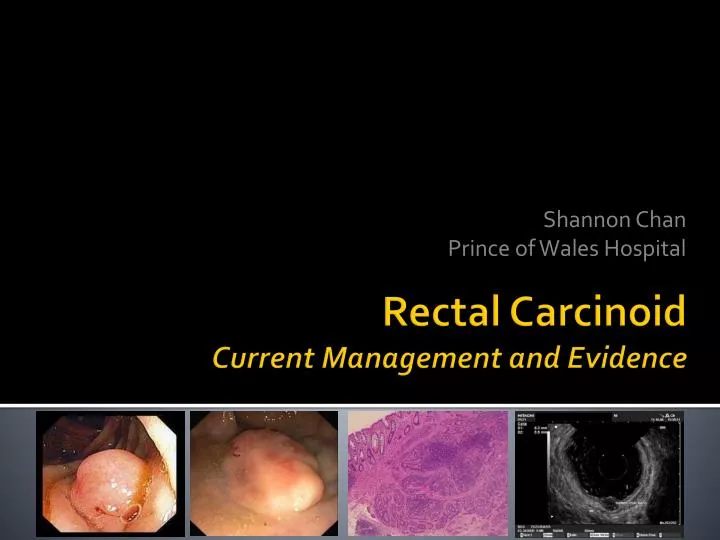
Shannon Chan Prince of Wales Hospital Rectal CarcinoidCurrent Management and Evidence
Case Scenario • F/47 Ms Ying • Good past health • Screening colonoscopy by private: • 1.5cm rectal polyp at 5cm from anal verge • Polyp base elevated with NS and snared • Path: Carcinoid, Margin involved
Concept Evolution 1907, Siegfried Oberndorfer described “carcinoid” (Karzinoide) of the small bowel at the German Pathological Society meeting Oberndorfer S. Karzinoide Tumoren des Dunndarms. Frank Z Pathol 1907
Concept Evolution 1963 Williams and Sandler classified carcinoids according to their embryologic site of origin as foregut carcinoids, midgut carcinoids, and hindgut carcinoids Pasieka et al.Surg Clin N Am 89 (2009) 1123-1137
Concept Evolution • 2000 WHO classification adopted the terms: • NE tumor • NE carcinoma Solcia E, Kloppel G, Sobin LH, et al. Histological typing of endocrine tumours. 2nd ed. WHO international histological classification of tumours. Berlin: Springer, 2000
Concept Evolution • “Carcinoid”, for gastroenteric NETs, used synonymously with the term ”well differentiated NE tumor” • “Malignant carcinoid” is used synonymously with the term well-differentiated NE carci- noma IRVIN M. MODLIN.Current Status of Gastrointestinal Carcinoids. GASTROENTEROLOGY 2005
5-yr Survival Rate (SEER Database) Small intestine: 5.5 - 43% Stomach: 21 - 74% Colon: 63 - 87% Rectum: 82 - 97% Feldman M, Friedman L, Brandt L. Sleisenger and Fordtrain’s Gastrointestinal and Liver disease. Philadelphia, PA: Saunders Elsevier; 2006 Laundry CS, Brock G, Scoggins CR, et al. A proposed staging system for rectal carcinoid tumors based on analysis of 4701 patients. Surgery 2008; 144:460-466
Epidemiology • 3rd most common gastrointestinal carcinoid tumor • 1.8% of malignant rectal tumor • Incidence 0.86/100 000 per year • 50 - 60y.o. • F : M = 1 : 1.1 • Asian and Afro-American • Black : White = 2.30 : 1 • Asian : non-Asian = 4.99 : 1 Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer. 2003;97(4):934-959
Presentation • 50% asymptomatic • Incidental finding during colonoscopy • Symptoms • Local symptoms: • Per rectal bleed • Change in bowel habit • Anorectal symptoms (tenesmus, discomfort, pruritus ani, pain) Consensus Guidelines for the management of patients with Digestive Neuroendocrine Tumors: Well-differentiated Colon and Rectum Tumor/ Carcinoma. Neuroendocrinology 2008; 87: 31-39
Presentation • Carcinoid syndrome: • Flushing & diarrhoea • Uncommon (<10%) • Usually biochemically inactive • Contain glucagon and glicientin • Metastasis (1.7 – 8.1%): • Abdominal pain • Hepatomegaly • Symptoms of carcinomatosis • Bowel obstruction: rare Consensus Guidelines for the management of patients with Digestive Neuroendocrine Tumors: Well-differentiated Colon and Rectum Tumor/ Carcinoma. Neuroendocrinology 2008; 87: 31-39
Diagnosis • Colonoscopy & biopsy • Smooth, round, submucosal nodule Jetmore AB, Ray JE, Gathright JB Jr, McMullen KM, Hicks TC, Timmcke AE. Rectal carcinoids: the most frequent carcinoid tumor. Dis Colon Rectum 1992;35:717-725
Diagnosis and staging • Endoscopic Ultrasound +/- FNAC: • Tumor size and depth of tumor invasion • Peri-rectal lymph node • Sensitivity: 87% Specificity: 93% (depth) Matsumoto T, Iida M, Suekane H, Tominaga M, Yao T, Fujishima M. Endoscopic ultrasonography in rectal carcinoid tumors: contribution to selection of therapy. Gastroinest Endosc 1991;37:539-542
Diagnosis and staging • MRI • Local invasion • Nodal involvement • Multi-slice triple phase CT Jetmore AB, Ray JE, Gathright JB Jr, McMullen KM, Hicks TC, Timmcke AE. Rectal carcinoids: the most frequent carcinoid tumor. Dis Colon Rectum 1992;35:717-725 Pelage JP, Soyer P, Boudiaf M, Brocheriou-Spelle I, Dufresne AC, Coumbaras J, Rymer R. Carcinoid tumors of the abdomen: CT features. Abdom Imaging 1999;24:240-245
Diagnosis and staging • 111In-Octreotide Scanning • Useful for determining metastatic disease • PET • DOPA or gallium-68 DOTA octreotate • FDG • 11C-5-hydroxytryptophan (5HTP) • Hoegerle S, Altehoefer C, Ghanem N, et al. Whole-body 18F Dopa PET for detection of gastrointestinal carcinoid tumors. Radiology 2001; 220:373–380. • Orlefors H, Sundin A, Garske U, et al. Whole-body 11C-5-hydroxytryptophan positron emission tomography as a universal imaging technique for neuroendocrine tumors: comparison with somatostatin receptor scintigraphy and computed tomography. J Clin Endocrinol Metab 2005; 90:3392–3400.
Diagnosis and staging • Lab tests • 24-hr urinary 5-HIAA –ve • Serum chromogranin A • Serum acid phosphate level • Pancreatic polypeptide • Enteroglucagon • B-HCG Kolby L, Bernhardt P, Sward C, Johanson V, Ahlman H, Forssell-Aronsson E, Stridsberg M, Wangberg B, Nilsson O: Chromogranin A as a determinant of midgut carcinoid tumour volume. Regul Pept 2004; 120: 269–273. 21 Ardill JE, Erikkson B: The importance of the measurement of circulating markers in patients with neuroendocrine tumours of the pancreas and gut. Endocr Relat Cancer 2003; 10: 459–462.
versus Local Resection Radical Surgery
Risk of Metastasis • Muscularis propria invasion • Atypia and high mitotic index Matsushita M, Takakuwa H, Nishio A. Management of rectal carcinoid tumors. Gastrointestinal Endosc 2003;58:641-642 Mani S, Modlin IM, Ballantyne G, Ahlman H, West B. Carcinoids of the rectum. J Am Coll Surg 1994;179:231-248
AJCC Cancer Staging Manual 7th edition 2010 Identical to the one proposed by ENETS in 2007 Rindi G, Kloppel G, Couvelard A, et al. TNM staging of midgut and hindgut (neuro) endocrine tumors: a consensus proposal including a grading system. Virchows Archiv. 2007;45:757-762
Treatment • Locoregional disease • Tumor size: • < 1cm: Endoscopic/ Transanal resection • 1.0 – 2.0: Controversial • > 2cm: Radical surgery (LAR+TME/ APR)
Results Shields CJ, Tiret E, Winter D. Carcinoid tumors of the rectum: A multi-institutional international collaboration. Annals of surgery; 252:750-755
Results • Tumor depth • Is NOT an independent risk factor Shields CJ, Tiret E, Winter D. Carcinoid tumors of the rectum: A multi-institutional international collaboration. Annals of surgery; 252:750-755
Results Shields CJ, Tiret E, Winter D. Carcinoid tumors of the rectum: A multi-institutional international collaboration. Annals of surgery; 252:750-755
Recommendations • Tumor size: • <1cm: Endoscopic/ transanal resection • 1.0 – 2.0cm: • Radical surgery (LAR+TME/ APR) • >2cm: Radical surgery (LAR+TME/ APR) • Lymphovascular invasion • Radical surgery (LAR+TME/ APR) Shields CJ, Tiret E, Winter D. Carcinoid tumors of the rectum: A multi-institutional international collaboration. Annals of surgery; 252:750-755
Metastatic Disease • Palliative Resection • Symptomatic relief • No survival benefit Schindl M, Niederle B, Hafner M, Teleky B, Langle F, Kaserer K, Schofl R: Stage-dependent therapy of rectal carcinoid tumors. World J Surg 1998; 22: 628–633.
Non-surgical Therapy • Somatostatin analogues • Interferon • Chemotherapy • Disappointing results • Radiotherapy • Not radiosensitive • Bone/ CNS metastasis De Herder WW. Tumours of the midgut (jejunum, ileum and ascending colon, including carcinoid syndrome). Best Pract Res Clin Endocrinol Metab 2005;19:705–715. Oberg K, Eriksson B. Nuclear medicine in the detection, staging and treatment of gastrointestinal carcinoid tumors. Best Pract Res Clin Endocrinol Metab 2005; 19:265–276.
Prognosis • Indolent disease • 5-yr survival rates: • Localised disease 84 – 90.8% • Regional spread 36.3 – 48.9% • Distant spread 20.6 – 32.3% Modlin IM, Lye KD, Kidd M: A five-decade analysis of 13,715 carcinoid tumors. Cancer 2003; 97: 934–959.
Conclusion • Indolent disease • Size dependent • Malignant potential • Surgery remains the mainstay of treatment • Ongoing trials for chemotherapeutic agents
1.5cm Rectal carcinoid with polypectomy done, margins involved So, going back to Ms Ying, what should we offer?