Download
1 / 55
590 likes | 793 Views
ORAL CAVITY TUMOURS. DR. JOJO V. JOSEPH MS. MCh (Onco) Chief Cancer Surgeon and Oncologist Division of Oncology Caritas Hospital, Thellakom, Kottayam. CANCERS OF ORAL CAVITY. High Incidence Easy to treat Metastasis Good results Field Cancerisation Improper treatment - MISERABLE LIFE.

E N D
ORAL CAVITY TUMOURS DR. JOJO V. JOSEPH MS. MCh (Onco) Chief Cancer Surgeon and Oncologist Division of Oncology Caritas Hospital, Thellakom, Kottayam
CANCERS OF ORAL CAVITY • High Incidence • Easy to treat • Metastasis • Good results • Field Cancerisation • Improper treatment - MISERABLE LIFE
HISTOLOGY • Sqamous Cell Carcinoma • Adenocarcinoma • Adenosquamous • Minor Salivary Gland Tumour • Soft Tissue Tumour • Bone Tumours • Rare Group
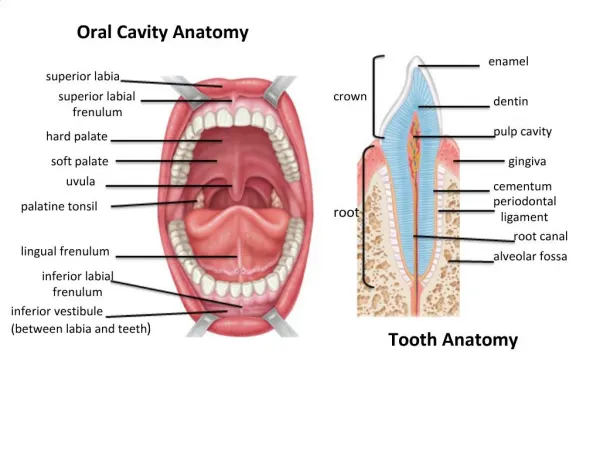
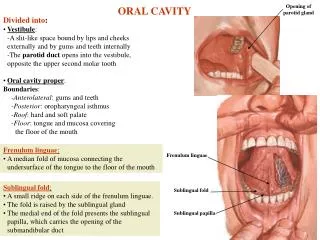
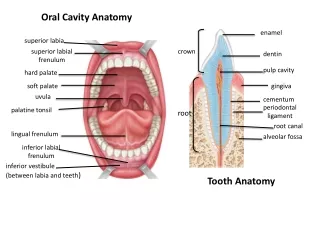
ANATOMY OF ORAL CAVITY • SUBSITES • Lips • Buccal Mucosa • Gingiva /Alveolar Margins • Floor Of Mouth • Oral Tongue • Soft and Hard Palates
LYMPHATIC DRAINAGE • Unilateral Drainage - > 250 nodes • Level I a -Submental Group • b -Submandibular group • Level II- From skull base to the level of Hyoid along IJV • Level III- From inferior border of Hyoid to Omohyoid • Level IV- Omohyoid to level of clavicle • Level V- Post.Triangle group • Level VI- Ant compartment, Hyoid to Supraclavicular ie Carotid to Carotid
STAGING OF THE DISEASE • Tx -Primary Tumour cannot be assessed • To -No evidence of Primary Tumour • Tis -Carcinoma in situ • T1 -< 2 cm in greatest dimension • T2 -2 - 4 cm • T3 -> 4 cm • T4 -Tumour invades adjacent structures.
N - Staging • Nx - Nodes cannot be assessed • No - No clinically positive nodes • N1 - Single Clinically positive < 3 cm • N2a- Single ipsilateral 3 to 6 cm • N2b- Multiple clinically positive ipsilateral nodes < 6 cm. • N3 - Clinically positive > 6 cm
DIAGNOSIS • Clinical Examination • Biopsy • OPG • Chest X-ray • DL Scopy/ Ba swallow + IDLE • CT Scan + MRI - Advanced/Recurrent.
PROGNOSTIC FACTORS • T. Stage • Tumour Thickness • < 2 mm 5% • > 5 mm 50% • N Stage • Nuclear atypia/DNA Content • Cytoplasmic Maturation • Tumour Angiogenesis • Molecular Markers.
TREATMENT • Primary Site • Lymph Nodes • Early Lesions -T1 and early T2 • Locally advanced - Bulky T2 - T4 • Recurrence / Residual Disease
OPTIONS • Local Treatment • Treatment for Lymph Node mets • Options: • Surgery • Radiotherapy • Chemotherapy • Combination
EARLY LESIONS • SINGLE MODALITY TREATMENT • SURGERY / RT • ADVANTAGES OF SURGERY • Whole specimen is made available for pathlogical analysis • Tumour Thickness • Less expensive • Shorter duration • Consider C Factor in Staging
CERTAINTY FACTOR • C1 -From standard diagnostic means • C2-With special diagnostic means • C3-Evidence from surgical exploration • C4-Evidence of Extent from definite Surgery • C5-Evidence from Autopsy
PRIMARY TUMOUR • WIDE EXCISION 5 MM MARGIN IN THREE DIMENSIONS • RECONSTRUCT THE DEFECT • PRIMARY CLOSURE • ALLOW SECONDARY HEALING • LOCAL ADVANCEMENT • SKIN GRAFT • FLAPS
LIPS UPTO 30% - V CLOSURE > 30% - FAN FLAP - MODIFIED FAN FLAP - KARAPANDZIC FLAP - ABBE-ESTLANDER FLAP
MANAGEMENT OF NECK • INCIDENCE OF NECK METASTASIS • T1 - UP TO 3% • T2 - 14 - 22% • T3 - 28 - 35% • T4 - >60%
NECK DISSECTION • COMPREHENSIVE NECK DISSECTION • RADICAL NECK DISSECTION. • MODIFICATIONS • SPINAL ACCESSORY • IJV • STERNOCLEIDOMASTOID
SELECTIVE NECK DISSECTIONS • SOHND • ANTERO LATERAL- I III IV • CENTRAL COMPARTMENT IDEAL • MODIFIED NECK DISSECTIONS • SELECTIVE - INCOMBINATION CASES
LOCALLY ADVANCED • WIDE EXCISION + NECK DISSECTION • LOCAL RADIOTHERAPY SURGERY FIRST • RADIATION ALONE IS NOT CURATIVE • CONSERVATIVE SURGERY IS POSSIBLE • MARGINS ARE BLURRED AFTER RT • MORBIDITY IS MORE • PROPER STAGING IS LOST • MORE EXTENSIVE SURGERY IS NEEDED
RECONSTRUCTION • SOFT TISSUE • BONE • SOFT TISSUE - FORE HEAD FLAP - MASSETER FLAP - DELTOPECTORAL - PECTARALIS MAJOR - STERNOMASTOID - LATISMUSADORSI - FREE FLAP
BONE • OSTEOMYOCUTANEOUS • RIB • CLAVICLE • FREE RADIUS • TIBIA