Download

1 / 48
480 likes | 787 Views
ORAL CAVITY MASS. Mangubat , Mary Love Joy Mansukhani , Sujata May Manzana , Apple. 38 y/o Male Chief complaint: Oral ulcer. History of Present Illness. Review of Systems (-) Past Medical History (-). Personal and Social History. 10 pack year smoking history

E N D
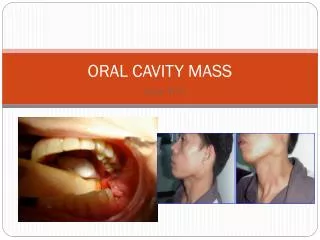
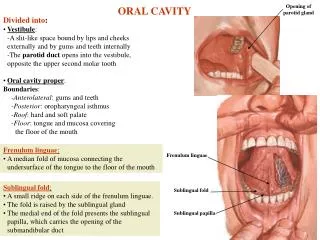
ORAL CAVITY MASS Mangubat, Mary Love Joy Mansukhani, Sujata May Manzana, Apple
38 y/o Male • Chief complaint: Oral ulcer
Review of Systems (-) • Past Medical History (-)
Personal and Social History • 10 pack year smoking history • (+) alcoholic beverage drinker
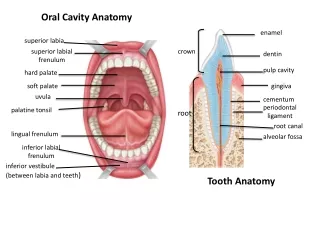
Physical Examination • Oral cavity: 2x2cm ulcer, lower gingiva near the retromolar trigone
Physical Examination • Neck: 4x4cm firm well-delineated, slightly movable mass at the left jugulo-digastric area -3x3cm firm, well-delineated, movable mass at the lower third of the SCM
Physical Examination • Thyroid gland: Negative for masses
Salient Features • 38 y/o Male • 10 pack year smoking history • (+) alcoholic beverage drinker • 2x2cm ulcer, lower gingiva near the retromolartrigone • 4x4cm firm well-delineated, slightly movable mass at the (L) jugulo-digastric area • 3x3cm firm, well-delineated, movable mass at the lower third of the SCM • thyroid gland: (-) mass
Differential Diagnosis • TB adenopathy • Metastatic carcinoma from oral cavity cancer • Lymphoma • Lymphadenitis from aphthous ulcer
Metastatic CA from ORAL CAVITY CA • SCC is the most common type (>90%) • Risk factors: alcohol and tobacco use, • Symptoms: non healing wound, pain, “on and off” bleeding , pain in swallowing, ear pain, a change in speech, uncoordinated swallowing, or a lump in the neck • sores in the mouth, whether they are related to trauma or to a variation of canker sores, should fully heal within three weeks http://www.headandneckcancer.org/patienteducation/docs/oralcavity.php
Metastatic CA from ORAL CAVITY CA • 80 % of unilateral neck mass are cervical metastasis from HNSCC • Oral cavity CA metastasize to the nodes in the ff levels: • Level 1 -submental,submandibular nodes • Level 2 –upper jugular chain nodes • Level 3 –middle jugular chain nodes Schwartz’s Manual of Surgery 8th Ed.
Lymphadenitis from Aphthous ulcer • Aphthous ulcer • Also referred to as canker sore, painful, open sore in the mouth; white or yellow and surrounded by a bright red area • they are benign • inner surface of the cheeks and lips, tongue, soft palate, and the base of the gums • emotional stress, dietary deficiencies (especially iron, folic acid, or vitamin B-12), menstrual periods, hormonal changes, food allergies, most commonly with viral infections
Lymphadenitis from Aphthous ulcer • may also be linked to problems with the body's immune system, mouth injury due to dental work, aggressive tooth cleaning, or biting the tongue or cheek • SYMPTOMS: tingling or burning sensation, pain, less common symptoms are fever, malaise, swollen lymph nodes
Lymphadenitis from Aphthous ulcer • complete healing in 1 to 3 weeks • large ulcers (>1 cm) take 2 to 4 weeks to heal • may recur monthly or several times a year http://www.nlm.nih.gov/medlineplus/ency/article/000998.htm
Lymphoma • Ulcers in the gingiva, tongue, palate, and tonsillar area • Clinical features: Elevated,ulcerated area that may proliferate rapidly, giving the appearance of traumatic inflammation • underlying HIV infection Harisson’s Principles of Internal Medicine 17th ed. Vol 1 p217
TB adenopathy • Metastatic carcinoma from oral cavity cancer • Lymphoma • Lymphadenitis from aphthous ulcer Metastatic Carcinoma from Oral Cavity CA
Thorough Physical Examination • visual inspection of the oral and nasal cavities, neck, throat, and tongue using a small mirror and/or lights • also feel for lumps on the neck, lips, gums, and cheeks • complete head and neck examination with indirect nasopharyngeal and laryngopharyngeal mirror examination
Endoscopy • use a thin, lighted tube called an endoscope to examine areas inside the body • type of endoscope to be used will depend on the area being examined • Laryngoscope - inserted through the mouth to view the larynx; • Esophagoscope - inserted through the mouth to examine the esophagus • Nasopharyngoscope- inserted through the nose so the doctor can see the nasal cavity and nasopharynx
Biopsy • TOLUIDINE BLUE- recommended for early detection as a guide for optimal biopsy. It clinically stains malignant lesions dark blue but does not stain normal mucosa. Dye is absorbed by the nuclei of malignant cells with increased DNA synthesis. • Follow with FNAB for cytology or excisional biopsy • If the diagnosis of carcinoma is made, endoscopic examination should proceed under general anesthesia with random biopsies of Waldeyer ring, the hypopharynx, nasopharynx, and other common sites of metastasis and any suspicious lesions • Subglottis, esophagus, and tracheobronchial tree are routinely evaluated to rule out synchronous primaries, which may have an incidence of 20%.
Routine hematologic examination • assess overall medical condition and possibility of spread to distant organs • Anemia may be detected with a CBC with platelet count • Liver function test determines hepatic spread
FINDINGS Nasopharyngolaryngoscopy (-) Biopsy of ulcer: Well-differentiated Squamous Cell Carcinoma Fine needle Biopsy of the neck mass: Chronic Lymphadenitis
Open Lymph node Biopsy • makes a cut in the skin and removes the lymph node • If more than one lymph node is taken, the biopsy is called a lymph node dissection • Open biopsy and lymph node dissection takes a bigger sample than a needle biopsy • Done to check to see if a known cancer has spread to the lymph nodes (staging) and to plan cancer treatment
Metastatic work ups, Imaging of oral cavity and neck to determine resectability • Chest radiograph PA and Lateral • Panoramic view (Panorex) of the mandible and/or dental X-rays. • When necessary to adequately assess the status of the patient's dentition • RULE OUT (1) A synchronous pulmonary tumor, (2) Acute or chronic pulmonary disease (3) Metastatic tumor. • Abnormal findings on chest x-ray or suspicious lesions need further imaging including a chest CT.
Metastatic work ups, Imaging of oral cavity and neck to determine resectability • CT and MRI of the head, neck and superior mediastinum • assess the presence and extent of nodal metastases, their relationship to the carotid and other adjacent structures, and to evaluate the superior mediastinum • also useful to identify abnormalities in the base of tongue and nasopharynx that may suggest the location of the primary tumor, and to rule out parapharyngeal or paratrachealadenopathy
Metastatic work ups, Imaging of oral cavity and neck to determine resectability • should also include the lung fields and liver for assessment of distant spread • Overall accuracy of nodal staging with CT (90-95%) appears superior to the accuracy obtained by clinical nodal staging (75-80%). Thus, more metastases are detected when CT is incorporated into the staging protocol of patients with primary head and neck squamous cell carcinoma
Metastatic work ups, Imaging of oral cavity and neck to determine resectability • MRI of the head and neck with or without Gadolinium • Including the nasopharynx, skull base, and neck, to attempt to locate the primary tumor within the nasopharynx and, if present, assess invasion of adjacent structures, such as the paraspinal muscles, infratemporalfossa, temporal bone, sphenoid sinus, bone marrow of the clivus, carotid artery, cranial nerves, and intracranial structures • overall accuracy in staging LN same with CT • preferred method for staging SCC of the oral cavity and oropharynx
Metastatic work ups, Imaging of oral cavity and neck to determine resectability • Panoramic x-ray (Panorex) of the mandible and/or dental X-rays. • When necessary to adequately assess the status of the patient's dentition in anticipation of radiation therapy. • PET scanning • additional diagnostic tool to improve the accuracy of CT • In early radiologic studies, combination of CT and PET has resulted in improved accuracy of staging, but this is not yet the standard of care
Proceed with Surgery • Standard for treatment of head and neck cancer • literature reports radiation therapy for patients with N0 or N1 necks and concludes that radiation or surgery can treat them equally well
Refer for radiation therapy • Nearly all patients with advanced disease require adjuvant radiotherapy, preoperatively or postoperatively • Preoperative radiotherapy has the risk of increased complications of surgery • Radiation dosage in excess of 6000 cGyis recommended with a boost to areas of high risk • Indications: • include a bulky tumor with significant risk of recurrence (T3 and T4) • histologically positive margins • perineural or perivascular invasion of tumor
Refer for radiation therapy • INDICATIONS FOR NECK: • elective treatment of the N0 neck not treated surgically where risk of micrometastasis is high • gross residual tumor in the neck following neck dissection • multiple positive lymph nodes • extranodal extension of tumor
FINDINGS Head and neck examinations: (-) Chest X-ray: (-) Panoramic x-ray of mandible: lytic lesion of the body of the mandible near the angle
Operative findings: • 3 x 2 cm ulcer of the lower gingiva with invasion into the mandible • 5 x 4 cm well-encapsulated firm mass located at the submandibular triangle (level 1 to level 2 ) • Multiple pinkish-red, firm, grossly enlarged nodes (1-2 cm) along the jugular chain (levels 2 to 4) • 4 x 3 cm well encapsulated firm mass at the subclavicular area
TNM Staging N T M
Operation done • Wide excision of the ulcer with segmental mandibulectomy with modified radical neck dissection, left: the defect was reconstructed using titanium plates.
Segmental Mandibulectomy • removes an entire segment of the mandible, disrupting continuity of the bone. This is performed when tumor invades bone. • may be performed in the setting of a composite resection, • resection of a segment of mandible in continuity with a cancer of the oral cavity or oropharynx or a primary cancer of the alveolar ridge. http://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&decorator=none&eid=4-u1.0-B978-1-4160-2445-3..50037-6&isbn=978-1-4160-2445-3
Advantages • Adequate margins of resection • Excellent exposure • Ease of exposure • Disadvantages • Cosmetic and functional consequences
Final histopath: • Well differentiated squamous cell carcinoma with metastasis to 5/20 lymph nodes, the largest measures 2 cm with extracapsular invasion; margins clear; with bony invasion
Radiation • Pre and post-op radiation • Improves local/regional control in HNSCC • within 6 weeks of surgery • 50 to 70 Gy over 5 to 7 weeks • Adverse reactions: • acute: mucositis, skin erythema • Late: fibrosis, xerostomia, altered state
Chemotherapy • No survival advantage compared to surgery and/or radiation • Cisplatin, carboplatin, 5-FU • Palliation of recurrent or unresectable disease, combined with radiation