Download
1 / 13
130 likes | 145 Views
Learn about coordinating home care for pediatric palliative care patients with chronic complex conditions. Address patient needs, discharge planning, and readmission prevention practices effectively.

E N D
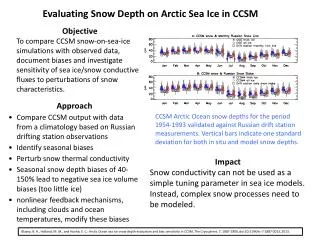
National Hospice and Palliative Care Organization’sPediatric Chronic Complex Conditions : Best practice for Home Care Coordination Susan M. Huff, RN, MSNSenior Director Johns Hopkins Pediatrics at Home
Objective • Understand the needs of chronic complex conditions (CCC) in pediatric palliative care patients. • Describe five areas you must address for effective patient discharge to home. • Explain best practices to prevent frequent unplanned hospital readmissions.
Johns Hopkins Pediatrics at Home (PAH) • 2,000 new patients served each year • Recent audit found 65% of patients have 1 diagnosis meeting needs for palliative care • 40% of patients have 2 palliative care diagnoses • Complex patients – readmission rate of 8% • No benchmarks • Comparison to adult readmission rate 24%
Serving CCC Patients: What We Know • Receive health care across settings • Day to day care relies on technology • Use multiple medications – frequent hospitalizations • Represent patients eligible for palliative care and hospice
Serving CCC Patients: What We Know • Move in and out of acute care facilities • Require intensive planning for discharge home • 5,000 children are within 6 months of life on any given day • 15,000 children die annually from conditions that could benefit from palliative care
Assessment • Assess families early in admission process • Work with family, hospice or home care organization to plan a safe discharge home • Assess family unit, culture, decision making process, communication styles, home environment, basic demographics.
Assessment • Families and patients should be involved in discharge planning and setting goals of care • Most pre-planning is for patients with high tech equipment • Ventilators, respiratory equipment, infusion and enteral therapy
Medication Management • Medication reconciliation • Pharmacist review medications with patient and family prior to discharge • Nurse training in medication reconciliation • Teach and monitor compliance at home • Discuss at every home visit
Teaching Parents/Caregivers • Simulation teaching and teach back • Use of interpreter • Videos for non-English speaking • Bedside and simulation out of patients room
Establishing Home Visit Frequency • Initial discharge to home - increased frequency of home visits • Teaching, building confidence, partnering with home health or hospice, providing support • Will improve overall compliance and lower unplanned readmissions
Communication Post-Discharge • Clear and frequent communication with case manager/home care coordinator prior to discharge • Information taken from hospital chart must be reviewed with patient and family • Once home, welcome calls
Conclusion • Vulnerable population – unavoidable readmissions • Goal is to ensure safe discharge and avoid frequent readmissions to a facility • Back to school, life, play, finding joy, quality of life • Supporting families to provide care and build trust
References • Feudtner C, Christakis DA, Zimmerman FJ, Muldoon JH, Neff J, Koepsell TD. Characteristics of deaths occurring in children’s hospitals: Implications for supportive care services. Pediatrics. 2002;109(5):887-893. • Savithri, N. and Golden, S. L. Factors Associated With the Stability of Health Nursing Services For Children With Medical Complexity. Home Healthcare Now.2017;35(8):434-444.