Download
1 / 60
630 likes | 1.03k Views
Hematopathology. Ruth Padmore MD, FRCPC, PhD Staff Hematopathologist The Ottawa Hospital. Lecture/Laboratory Outline. Hematopathology Lecture (9 - 10:15am) Basic Histology, text and atlas, LC Junqueira and J Carnerio, 11 th edition, McGraw-Hill, 2005, ISBN 0-07-144091-7

E N D
Hematopathology Ruth Padmore MD, FRCPC, PhD Staff Hematopathologist The Ottawa Hospital
Lecture/Laboratory Outline • Hematopathology Lecture (9 - 10:15am) • Basic Histology, text and atlas, LC Junqueira and J Carnerio, 11th edition, McGraw-Hill, 2005, ISBN 0-07-144091-7 • Chapters 12 (Blood cells), 13 (Hematopoiesis) and 14 (Lymphoid organs) • Stem cell transplantation 10:15 – 10:30 BREAK • Histology Laboratory (10:30am - noon), Room 2236 • Review glass slides of: • Normal peripheral blood and bone marrow • Selected diseases
Lecture Outline • Hematopathology Lecture • Basic Histology, text and atlas, LC Junqueira and J Carnerio, 11th edition, McGraw-Hill, 2005, ISBN 0-07-144091-7 • Chapter 12: Blood Cells • Chapter 13: Hematopoiesis • Chapter 14: Lymphoid Organs
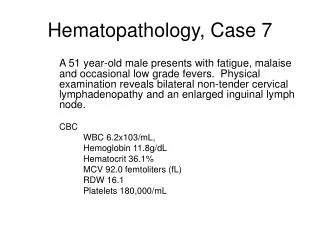
Peripheral Blood • About 55% of blood is liquid • The liquid portion of blood (before clotting) = plasma • The liquid portion of blood (after clotting) = serum • The cellular part of blood (45% of volume) is made up of a variety of different cell types • The hematocrit (Hct) measures the volume occupied by the cells in the blood Figure 12-1
Cellular Components of Blood • Erythrocytes • Also called red blood cells (RBCs) • Leukocytes • Also called white blood cells (WBCs) • 5 majors types: • Neutrophils (60%) • Lymphocytes (30%) • Monocytes (7%) • Eosinophils (2%) • Basophils (1%) • Platelets • Also called thrombocytes
Figure 12-3. Scanning Electron Micrograph of normal human erythrocytes. Note their biconcave shape for maximum oxygen exchange. x 3300 Wright-Giemsa stained Peripheral blood film In mammals, RBCs in peripheral blood lack a nucleus; whereas those of birds and reptiles have a nucleus.
Erythrocytes (Red Blood Cells) • RBCs contain mostly hemoglobin, to carry oxygen to the tissues • One hemoglobin molecule can carry 4 oxygen molecules
Figure12-4. Scanning electron micrograph of a sickle cell, from a person homozygous for the sickle cell mutation (Glu to Val in position 6 of beta chain of the hemoglobin molecule)
Figure 12-5. The five types of Human Leukocytes • The 5 types of WBCs • Can be identified by automated hematology analyzer (5 part differential count) • Neutrophils (60%) • Lymphocytes (30%) • Monocytes (7%) • Eosinophils (2%) • Basophils (1%)
Figure 12-6. Neutrophils, Giemsa-stained • Neutrophils are also called polymorphonuclear leukocytes, due to the multiple number of nuclear lobes • Barr body (drumstick like nuclear appendage) = inactivated X chromosome in females (see diagram fig 12-5)
Abnormal Neutrophils • Hypersegmented neutrophils: a sign of Vitamin B12 or folate deficiency (interferes with DNA synthesis) • Hyposegmented neutrophils (Pelger-Huet like morphology) a sign of myelodysplasia)
Neutrophil Granules • Substances present in both primary and secondary granules: • Collagenase, lysozyme • Primary (azurophilic) granules • Larger (0.5um) than secondary granules • Contain myeloperoxidase, acid phosphatase and other enzymes • Secondary (specific) granules • Lactoferrin (binds iron), alkaline phosphatase
Destruction of Bacteria by Neutrophils • Neutrophil engulfs bacteria • Bacteria in vacuoles (phagosomes) in neutrophils • Specific granules fuse with and discharge contents into phagosome • pH of phagosome lowered to 5.0, for maximal activity of lysosomal enzymes • Azurophilic granules discharge contents into phagosomes, killing and digesting bacteria • Absolute neutrophil count (ANC) is normally between 2 to 5 x 109/L • If neutrophil count less than 0.5 x 109/L, at high risk for bacterial sepsis (febrile neutropenia) • Increased neutrophils in peripheral blood as response to infection = neutrophilia
Eosinophils: Figures 12-8 and 12-9 • Bilobed nucleus • Prominent eosinophilic (reddish) granules • Same size or just slightly larger than neutrophils (12-15um in diameter) • Eosinophilia: • Allergic reactions • Asthma • Drug reactions • Parasitic reactions
Figure 12-12 Basophils • Rare in peripheral blood (less than 1%) • Similar in size to neutrophil (12-15um) • Nucleus divided into irregular lobes which are obscured by overlying specific granules, which contain heparin and histidine • Noted in hypersensitivity reactions
Figure 12-15: Lymphocytes • Range from small lymphocytes, 6-8um diameter, to large lymphocytes up to 18um diameter • Round nucleus, with coarsely clumped chromatin • scant blue cytoplasm, with rare azurophilic granules • Function in immune reactions, defending against microorganisms, foreign macromolecules, and cancer cells
Flow Cytometric ImmunophenotypicAnalysis of Leukocytes Cells gated based on Forward Scatter, FS (cell size) and Side Scatter, SS (cell granularity) Fluorescent-tagged antibodies identify lineage of cells (T-cell, B-cell, myeloid)
Flow Cytometric ImmunophenotypicAnalysis of Leukocytes • T-cells: • CD2, CD3, CD4, CD5, CD7, CD8 • Kill virus infected cells • Recruit B-cells in immune response • B-cells • CD19, CD20, CD22, surface kappa, lambda • Differentiate into plasma cells and make antibodies • NK-cells • CD2, CD56 • Killing of tumour and virus-infected cells
Figure 12-17: Monocytes • Large cells, 12-20um, with kidney-shaped nucleus and abundant bluish-grey cytoplasm • Enter tissue and differentiate into macrophages • Phagocytic function
Platelets • Small, non-nucleated fragments of cytoplasm formed from megakaryocytes in bone marrow • 2-4um diameter, disc-shaped • 200-400 x 109/L in peripheral blood • Life span 10 days in peripheral blood
Figure 12-19: Electron micrograph on human platelet • Prevent bleeding • Repair gaps in blood vessel walls • Promote blood clotting • Open canalicular system for rapid release of active molecules in clotting • Microtubules, actin, myosin function in changes of shape (discoid to ameboid)
Figure 12-19: Electron micrograph on human platelet • Alpha granules • Fibrinogen, PDFG • Dense granules • ADP, ATP, Ca++, serotonin • Clotting: • Platelet aggregation • Blood coagulation • Clot retraction • Clot removal
Hematopoiesis • Hematopoiesis: making blood cells • Location of hematopoiesis: • Embryo: yolk sac, then liver/spleen • After birth: bone marrow • Types of hematopoiesis: • Erythropoiesis: red cells • Granulopoiesis: granulocytes • Megakaryopoiesis: megakaryocytes
Hematopoietic cells during differentiation Figure 13-1 • Stem cells: • Rare cells, proliferate at low level, self-renew • Pluripotential stem cell • Lymphoid multipotential cell, Myeloid multipotential cell • Progenitor Cells • Source of differentiated cells, influenced by growth factors, reduced multipotentiality • Colony forming cells ( or units, CFC or CFU), • eg. CFU-E: erythrocyte-colony forming cell or unit • Precursor Cells (blasts) • High mitotic activity, lineage committed • Eg Lymphoblast, erythroblast etc. • Mature cells • No mitotic activity, abundant in peripheral blood
Hematopoiesis: Recombinant Growth Factors in Clinical Use Table 13-2 • G-CSF: (Neupogen, Filgastrin) • Stimulated formation and function of neutrophils and neutrophil precursors • Used in cases of febrile neutropenia following chemotherapy for cancer • Avoid use in acute myeloid leukemia, stimulates leukemia blasts to grow • Erythropoietin: (epoetin alpha, EPO, darbepoetin alpha) • Produced by kidney in response to hypoxia • Stimulates erythropoiesis, prevents apoptosis of erythroid precursors • Used in renal dialysis patients to prevent anemia and cancer patients to improve quality of life • side effects: hypertension, thrombosis, pure red cell aplasia due to anti-EPO antibodies, changed formulation to reduce antigenicity
Figure 13-3. Section of Hematopoietically Active Bone Marrow • Connective tissue stroma • Hematopoietic cords • Sinusoids
Stages in Red cell (erythroid) Maturation Proerythroblast Basophilic Polychromatic Orthochromic erythroblast erythroblast erythroblast (two examples)
Figure 13-7: Erythropoiesis Aspirate Biopsy
Stages in Granulocyte Maturation Blast cell Promyelocyte Myelocyte Metamyelocyte Band cell Segmented Neutrophil
Figure 13-9. Granulopoiesis Aspirate Biopsy
Mature megakaryocytes form by cell division without nuclear division Megakaryocytes are polyploid, 8 to 16 ploidy and very large 35-150um Figure 13-16:Megakaryopoiesis and Platelet Formation Megakaryocyte in aspirate Several megakaryocytes in bone marrow biopsy
The Immune System • Function of the immune system: to eliminate foreign molecules/cells (tumor cells, virally infected cells, bacteria, foreign bodies) • Two basic types of immune response: • (1) innate response: • Neutrophils • Macrophages • Mast cells • Natural killer cells • (2) adaptive response: (lymphocytes) • B-cells • T-cells
Chapter 14: Lymphoid Organs • Cells of the immune system are organized into lymphoid organs • (1) distributed through body in blood, lymph, and epithelial and connective tissues • (2) lymphoid nodules • (3) lymphoid organs • Lymph nodes • Spleen • Thymus • Bone marrow
The adaptive immune response:B-cells (Humoral response) • B-cells are activated by foreign proteins (antigens) and differentiate into plasma cells • Plasma cells make immunoglobulin Figure 14-24A: Plasma cells in medulla of lymph node
Table 14-1:Classes of Immunoglobulins (Ig) • IgG: monomer, lots of it in plasma, neutralizes antigens • IgM: pentamer, initial immune response, high levels seen in acute infection • IgA: dimer, present in secretions (saliva, breast milk, tears), protects mucosal surfaces • IgE: monomer, allergic and anti-parasite responses • IgD: monomer, small amount in plasma, triggers initial B-cell activation
Antibodies • Microorganism is covered by antibodies that recognize it (opsonization) • Antibody-coated microorganism is ingested by macrophages, neutrophils, eosinophils, which have receptors for the FC part of the immunoglobulin molecule • IgM activates the complement system • C3 binds to microorganism, and is ingested by phagocytic cells with C3 receptors • Complement cascade produces membrane attack complex, makes holes in cell membrane, resulting in cell lysis
The adaptive immune response:T-cells (Cellular response) • T-helper Cells • CD4+, receptor for class II MHC molecules • Class II MHC molecules expressed by antigen presenting cells (B-cells, macrophages, dendritic cells), which present exogenous antigen to the T-helper cell • T-helper cell is stimulated to: • Make B-cells differentiate into plasma cells • Activate cytotoxic CD8+ T-cells • Induce an inflammatory reaction
The adaptive immune response:T-cells (Cellular response) • T-cytotoxic Cells • CD8+, receptor for class I MHC molecules • Class I MHC molecules expressed by almost all cells in the body • Class I MHC molecules complex with abnormal endogenous proteins (eg virally infected cell or tumour cell) • This complex is presented to the CD8+ T-cytotoxic cell, resulting in: • Release of perforins with destruction of abnormal cell • Induce apoptosis of abnormal cell
Mucosa-Associated Lymphoid Tissue (MALT) • Lungs • Peyer’s patches (small bowel) • Tonsils • Sites of IgA secretion to protect mucosal surfaces from infection Figure 14-12: Palatine Tonsil
Figure14-14.Thymus with lobules composed of dark cortical and light medullary zones • Thymus is site of T-cell differentiation, into CD4+ or CD8+ T-cells • Thymic-blood barrier, with non-fenestrated endothelial cells • No afferent lymphatics
Figure 14-20.Schematic of Lymph Node Figure 14-21.Section of Lymph Node Hematoxylin & Eosin stain (H&E)
Figure 14-35. Spleen macrophages with phagocytosis of red cells (erythrophagocytosis) Figure 14-33. Scanning electron micrograph of sinusoids, red pulp cords and macrophages
Stem Cell Transplantation • CD34+ hematopoietic stem cells used in transplantation • Three sources of stem cells: • peripheral blood, bone marrow or cord blood • Autologous Transplant: • Stem cells are collected from the patient, and re-infused after intensive chemotherapy and radiation therapy • Allogeneic Transplant: • Stem cells are collected from a donor, and are infused into the patient after intensive chemotherapy and radiation therapy
Stem Cell Transplantation • Complications of Stem Cell Transplantation • Failure of engraftment • Relapse of malignancy • Graft-versus-host disease
Complications of Stem Cell Transplantation:Graft-versus-host Disease (GVHD) • Stem cell transplants are HLA-matched • 6/6 match, identical for HLA-A, B and DR • GVHD develops after successful engraftment, as engrafted donor immune system recognizes recipient tissues as foreign • Can be acute or chronic • Organs affect: skin, liver, gut, eye, oral (dry mouth)
Other forms of GVHD:Passenger Lymphocyte Syndrome • Seen in solid organ transplant (e.g. kidney) • Donor has antibodies to recipient red cell antigens • Hemolysis develops after transplant, due to donor lymphocytes present in the blood vessels of the donated organ • May result in transient hemolysis and anemia after transplant
Other forms of GVHD:Transfusion related Graft-versus-host Disease • Lymphocytes can engraft after blood transfusion • If donor and recipient are haplo-identical for HLA (3/6 match) • Donor lymphocytes engraft because of haplotype match, but then recognize recipient as foreign, because of haplotype mismatch • Recipient bone marrow cells are destroyed, resulting in pancytopenia • Is always fatal due to bone marrow failure