Download
1 / 62
620 likes | 645 Views
Learn about the limitations and management strategies for calcium channel antagonist toxicity in children. Understand the pharmacology, physiological effects, and treatment options.

E N D
Calcium Channel Antagonists in Children Rama B. Rao, MD NYU/Bellevue Hospital Center 2007
Physiology of Children • GI • Lower hepatic glycogen reserves • Limited enzymatic capacity • pH and motility • Chew or bite tablets altering absorption
Physiology of Children • Respiratory • Diminished reserves • Metabolic • Increased requirements
Management Limitations • No confirmatory assay • Qualitative • Quantitative • Delayed onset toxicity
Limitations • Therapeutic interventions • No antidote • Variable outcomes • Limited data in children
Pharmacology of CCA • Most tablets exclusively dosed for adults • Often slow release • Hepatically metabolized
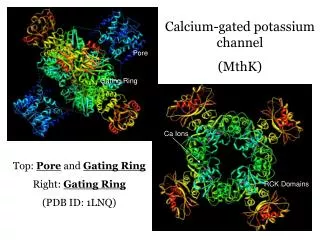
Calcium Channels • L type: Myocardium, sm mm, ß Islet pancreas • T • N • P Neuronal, SR, other • Q • R
NORMAL MYOCARDIAL CELL Ca2+ 3 SR 4 PKA Ca2+ 5 ATP cAMP 2 AC Gs ß1 1
CCA Ca2+ 3 SR 4 PKA Ca2+ 5 ATP cAMP 2 AC Gs ß1 Result: Negative inotropy 1
Contractile Cells 1 Phase 2 Myocardial Cell Ca2+ inward (with K+ outward) 2 0 3 4 4 Result CCA: Diminished contractility
Pacemaker Cells 1 Phase 2 Myocardial Cell 2 Phase 4 Purkinje Fiber SA Node 0 3 4 4 Result CCA: Altered conduction Delayed initiation Depressed movement thru Purkinje fiber
Vascular Smooth Muscle Ca2+ Voltage sensitive Ca2+ Calmodulin Receptor operated 1 Contraction of sm mm Ca2+
CCA and Vascular Smooth MM Ca2+ Voltage sensitive Ca2+ Calmodulin Receptor operated 1 Result : reduced vasoconstriction Ca2+
CCA: Dihyrdopyridines Smooth mm: peripheral vasodilation • In mild overdose: • Hypotension • Tachycardia • In children and severe OD • Hypotension • Bradycardia
CCA: Verapamil, CardizemPhenylalkylamines • Greater binding at myocardial cells • Negative inotrope • Negative chronotrope • Inhibit release of insulin in overdose
CCA: Management • Assume ingestion • Assess early/late or imminent* • IV, ECG, monitoring *Fingerstick blood glucose?
Decontamination • Activated charcoal: 1 gm/kg • MDAC: 0.5 gm/kg q4 • Whole bowel irrigation?
Fellowship Case • 30 month old male is found with an open bottle of verapamil SR 240mg tabs. • New Rx : 100 tabs • 94 tabs found
Case continued • Toddler has normal vital signs • Playful • Running around the ED
Whole Bowel Irrigation • PEG balanced salt solution • Assess for bowel sounds • NGT placement with confirmation • First AC • Follow with PEG 500* ml/hr (start at 100 ml/hr and rapidly titrate) • Q4 AC • Continue until clear rectal effluent *Can give higher dose of up to 2L/hour as tolerated
Management Conundrums Hypotension: What can we try?
Ca2+ CCA and Vascular Smooth MM Ca2+ Voltage sensitive Ca2+ Calmodulin Receptor operated 1 Ca2+ Ca2+
Ca2+ CCA and Vascular Smooth MM Ca2+ Voltage sensitive Ca2+ Calmodulin Receptor operated 1 Ca2+ NE, Phenylephrine Ca2+
Rx: Vasodilation AgentVasoconstrictionHRCO NE ++++ ↓↓↓ PE ++++ ↓↓↓ HR = Heart rate; CO=Cardiac Output NE= Norepinephrine PE= Phenylephrine
Clinical Evaluation • Mental status • Peripheral circulation • Urine output • Lactate production • Acid/base status
Vasodilation • Crystalloid • Calcium: variable efficacy • Direct acting α1 agonists • Norepinephrine • Phenylephrine • Caveat need to combine with inotropes
Bradycardia What can we try?
Bradycardia • Atropine and calcium • Variable efficacy • ß1 agonists* • Direct: Epinephrine, Isoproterenol • Indirect: Glucagon
Bradycardia AgentVasoconstrictionHRCO Calcium ± ± ↑↑ Atropine↑± Isoproterenol↓ ↑± ↑± Glucagon↑± ↑± Epi± ↑± ↑±
Inotropes • Critical to cardiac output • Allow titration of pressors • Also have caveats
NORMAL MYOCARDIAL CELL Ca2+ 3 SR 4 PKA Ca2+ 5 ATP cAMP 2 AC Gs ß1 1
CCA Ca2+ Ca2+ 4 SR PKA Ca2+ Amrinone 5’MP ATP cAMP 3 AC Glucagon Gs 2 ß1 Epi, Dobutamine 1
Inotropes • ß1 agonists • Direct • Indirect • Phosphodiesterase inhibitors • Calcium
Calcium 10% = 100 mg/mL • Calcium chloride • 1.36 mEq/mL • Central line important • Calcium gluconate • 0.43 mEq/mL
CaCl2 10% (100 mg/mL) • 20 mg/kg bolus over 3-5 minutes • Repeat in 10 minutes • Dilute concentration to 20 mg/mL • 20-50 mg/kg/hr infusion
Calcium Gluconate 10% (100 mg/mL) • 60-100 mg/kg bolus over 3 minutes • (remember this has less mEq Ca2+) • May repeat in 10 minutes • Dilute to 50 mg/mL • Infusion 120-240 mg/kg/hr
Inotropes • ß1 agonists • Direct • Indirect • Phosphodiesterase inhibitors • Calcium
Inotropes AgentVasoconstrictionHRCO Dobutamine*↓ ↑± ↑ Epi ± ↑↑± ↑± Glucagon↑± ↑± Amrinone*↓ ↑ ↑ Calcium ±±↑ * Needs pressor
In CCA Toxicity AgentVasoconstrictionHRCO NE ++++ ↓↓↓ PE ++++ ↓↓↓ Calcium ± ± ↑↑ Atropine ↑± Isoproterenol↓ ↑± ↑± Dobutamine↓ ↑± ↑ Epi ± ↑↑± ↑± Glucagon↑± ↑± Amrinone↓ ↑ ↑ HR = Heart rate; CO=Cardiac Output
Insulin and Dextrose • Increase energy efficiency • Prolongs opening of Ca2+ channels • Potential anti-inflammatory effects
Insulin and Dextrose • Canine models • Increase lethal dose verapamil • Delayed time to death • Not necessarily change in heart rate or MAP • Compared to saline, epi, glucagon groups
Insulin and Dextrose • Human cases • No comparative trials • Often rescue medication • None as first line therapy • ?Reporting bias of success • At least a dozen survivors • Bolus vs infusion