Download

1 / 19
200 likes | 234 Views
Pain is a complex sensory and emotional experience, serving as a vital sign indicating issues. Learn about pain sources, types, duration, and management. Discover factors affecting pain experience and nursing interventions. Explore pharmacologic and nonpharmacologic pain relief methods.

E N D
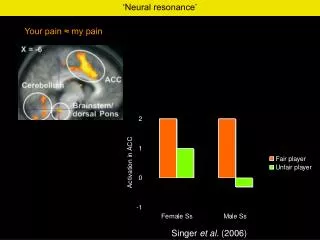
Pain • Is unpleasant sensory and emotional experience associated with actual and potential tissue damage. • It is considered the fifth vital sign. • It is one of the human body defense mechanisms that indicates the person is experiencing problem.
Sources of Pain • Nociceptive: pain that is usually transmitted after normal processing of noxious stimuli • Cutaneous (superficial): usually involves the skin or the subcutaneous tissue • Somatic: is diffuse or scattered and originates in tendons. • Visceral: is poorly localized and originates in body organs • Neuropathic: results from injury or abnormal functioning of peripheral nerves or CNS • Psychogenic: unknown physical cause
PHYSIOLOGY OF PAIN SOURCES Chemical/Thermal Injury, Inflammation Heat, Cold PAIN RECEPTORS (Nociceptors) Histamine, Bradykinin, Serotonin, E-prostaglandin DISCHARGE IMPULSES Electrical Activity to spinal cord and onto the Brain BRAIN = Electrical activity becomes the experience of PAIN
Duration of pain • Acute pain: generally rapid in onset, varies in intensity from mild to severe, lasts from brief period to less than 6 months • Chronic pain: may be limited, intermittent or persistent but lasts for 6 months or longer and interferes with normal functioning. • Remission: when the pain present but the patient does experience symptoms • Exacerbation: reappear of symptoms • Intractable pain: resistant pain to therapy, and persists despite a variety of interventions
Origin of Pain • Physical cause — cause of pain can be identified • Psychogenic — cause of pain cannot be identified • Referred — pain is perceived in an area distant from its point of origin
Perception of Pain • Pain threshold: is the lowest intinsity of stimulus that causes the subject to recognize pain • Adaptation • Modulation of pain • Neuromodulators • Endorphins, dynorphins enkephalins
Common Responses to Pain • Physiologic: ↑BP, ↑HR,↑RR, pupil dilation, muscle tension and tension rigidity, pallor, ↑adrenaline level, ↑blood glucose • Behavioral: moving from painful stimuli, grimacing, moaning, crying, restlessness, protecting painful area • Affective: exaggerated weeping, withdrawal, anxiety, depression, fear, anger, anorexia, fatigue, hopelessness, powerlessness.
Factors Affecting Pain Experience • Culture • Ethnic variables • Family, gender, and age variables • Religious beliefs • Environment and support people • Anxiety and other stressors • Past pain experience
General Assessments of Pain • Patient’s verbalization and description of pain • Duration of pain • Location of pain • Quantity and intensity of pain • Quality of pain • Chronology of pain • Aggravating and alleviating factors • Physiologic indicators of pain • Behavioral responses • Effect of pain on activities and lifestyle
Pain assessment tools WILDA Scale • Words that describe the pain • Intensity of pain • Location of pain • Duration of pain • Aggravating or alleviating factors
Diagnosing Pain • Type of pain • Etiologic factors • Behavioral, physiological, affective response • Other factors affecting pain process
Nursing Interventions for Pain • Establishing trusting nurse-patient relationship • Initiating nonpharmacologic pain relief measures • Considering ethical and legal responsibility to relieve pain • Teaching patient about pain
Manipulating Pain Experience Factors • Remove or alter cause of pain • Alter factors affecting pain tolerance • Initiate nonpharmacologic relief measures
Nonpharmacologic Pain Relief Measures • Distraction • Humor • Music • Imagery • Relaxation • Cutaneous stimulation • Acupuncture • Hypnosis • Therapeutic touch
Pharmacologic Pain Relief Measures • Analgesic administration • Nonopiod analgesics e.g. NSAIDs • Opioids or narcotic analgesics • Adjuvant drugs e.g. anticonvulsants, antidepressants, ..
Why clients may be reluctant to report pain: • Unwillingness to trouble staff who are perceived as busy • Fear of injectable route of analgesic administration • Belief that pain is to be expected as apart of the recovery process • Belief that pain is a normal part of aging • Belief that expression of pain reveal weakness • Concerns about side effects and risks especially of opioid drugs
Additional Methods for Administering Analgesics • Patient controlled analgesia • Epidural analgesia • Local anesthesia