Download
1 / 142
1.52k likes | 2.4k Views
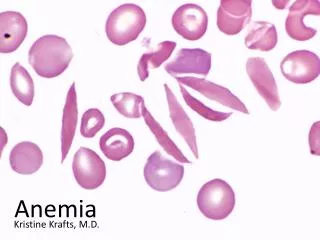
dr. Bastiana SpPK. Gangguan Eritrosit : Anemia. Anemia. Polisitemia. Gangguan Eritrosit. ANEMIA. Definisi Anemia: Sindroma klinis yang disebabkan penurunan massa eritrosit total dalam tubuh .

E N D
dr. BastianaSpPK GangguanEritrosit: Anemia
Anemia Polisitemia GangguanEritrosit Company Logo
ANEMIA Company Logo Definisi Anemia: • Sindromaklinis yang disebabkanpenurunanmassaeritrosit total dalamtubuh. • Keadaandimanamassaeritrositdanataumassa hemoglobin tidakdapatmemenuhifungsinyauntukmenyediakanoksigenbagijaringantubuh • Penurunandibawah normal kadarHb, hitungeritrosit, danhematokrit
ANEMIA PenurunanHbdanHct : < batasbawah 95% interval referens darikelompokusia, jeniskelamin danlokasigeografis (ketinggian) Anemia Hb12-14 g/dl ; (Hct 36-41%), Hb7g/dl symptom (+) Akut:hipovolumia (pucat, ggnpenglihatan, syncope, tachycardia) ; Kronis: tissue hypoxia (fatique, dyspnea, Headache, angina) Company Logo
ANEMIA → symptoms / syndrome • Hb↓ • PCV ↓Hypoxia → Otak , Otot • RBC ↓ Kompensasi : - heart rate ↑→ tachycardia → flow rate ↑ → cardiomegaly → heart failure → † - blood flow priority (pallor) - RBC 2,3-DPG content ↑→ O2 dissoc.curve shift to the right → O2 release to the tissues ↑ .
Klasifikasi Anemia Company Logo Berdasarkanpatofisiologi: I. Kegagalanproduksiseldarahmerah: A. Gangguanselindukhematopoesis Anemia Aplastik B. Gangguansintesis DNA Anemia Megaloblastik C. Gangguansintesis Hemoglobin (Hb) Anemia DefisiensiBesi, Thalasemia D. Gangguansintesiseritropoetin Anemia karena GGK
Lanjutan…..anemia berdasarkanpatofisiologi Company Logo E. Gangguankarenamekanisme lain: Anemia karenapenyakitkronis, anemia sideroblastik Anemia karenainfiltrasisumsumtulang II. Peningkatandestruksiseldarahmerah: Anemia Hemolitik III. Kehilangandarah (Blood Loss) Anemia karenaperdarahanakut
Anemia Company Logo Anemia berdasarkanmorfologi • Anemia sec. morfologieritrosit, dilihatdari: - ukurandanwarnadibawahmikroskopatau - indekseritrosit(MCV, MCH, dan MCHC) • KriteriaUkuran (size): Normositik, Mikrositik, Makrositik • KriteriaWarna (pucat): Normokromik, Hipokromik
Cara MengetahuiUkuraneritrosit: * membandingkandenganintisellimfositkecil(di bawahmikroskop) : → ukuransama = normositik lebihkecil = mikrositik lebihbesar = makrositik * MenghitungMCV(Mean Cell Volume) MCV= PCV/EryX 10 (fL) (1 fL=10-12L= 1μm3) N : dewasa = 80-100 fL , dibawah 1 thn = 76- 86 fL MCV : normositik , mikrositik, makrositik * Eritrositdenganvariasiukuran yang abnormal anisositosis
PerhatikanWarnaseleritrosit: - Bandingkan diameter central pallor(CP) dengan diameter seleritrosittersebut . - Normal, bentukseleritrositadalahseperticakram bikonkaf (biconcave disk) →padahapusandarahtepiterlihatbulat, Ø 7-8 μdenganarea central pallor dibagiantengah CP≤ 1/3 Ø Eri = normokromik CP> ½ Ø Eri = hipokromik
Eritrositdengancentral palor (CP) Bandingkan diameter CP dengan diameter seleritrosit
Warna, dapatdiketahuijugadariMCH(Mean Cell Hb) MCH= Hb/RBC x 10 (pg) Dewasa: MCH=27-32 pg, Anak-anak: MCH=23-31 pg (1pg=10-12g=1μμg) MCH normal → normokromik MCH < normal → hipokromik • MCHC (Mean Cell Hb Concentration) : MCHC=Hb/PCV x 100 (g/dL) Normal: MCHC = 32-36 g/dL
Anemia Hipokromik-Mikrositik. 1. Anemia Normokromik-Normositik 2. Anemia Makrositik 3. Klasifikasi Anemia secaramorfologi Company Logo
1 2 3 • Contoh: • - Anemia • defisiensi Fe • Thalasemia • Anemia akibat • PenyakitKronik • Anemia • sideroblastik • Contoh: • Anemia pasca • perdarahanakut • Anemia aplastik • Anemia hemolitik • Anemia akibat • penyakitkronik • Anemia pada GGK • Anemia pada • mielofibrosis • dll Megaloblastik, contoh: - Anemia defisiensiFolat, - Anemia defisiensi vitamin B12 B. Nonmegaloblastik contoh: - Anemia pd peny. Hatikronis - Anemia pd hipotiroid, dll Anemia hipokromik-mikrositik Anemia normokromik-normositik Anemia makrositik MCV 80 -95 fl MCH 27-34 pg MCV <80 fl; MCH <27 pg MCV > 95 fl Company Logo
Makrositik makrosit-oval (Anemia megaloblastikditandaiolehmakrosit oval ini)
Pendekatandiagnostik Anemia: • Anamnesis:onset /bleeding tendency / routine medicinal / occupation / hobby / travel history / family / diet / GI symptoms / menstruation cycle / history of previous pregnancy-delivery / alcohol consumption , etc • Pemeriksaanfisik:conjunctiva & lips (pallor) / mouth (cheilosis) / tongue (glossitis) / gum / nails (koilonychia) , hair (signa de bandera, alopecia) , jaundice , petechiae , liver & spleen , lymphenodes ,rectal / vaginal toucher, feet (ulcer,arthritis)
PemeriksaanLaboratorium - CBC (complete blood count )→ to confirm anemia (Hb, PCV, RBC) & the type of anemia (MCV; MCH; MCHC), RDW - Reticulocyte count → reflects marrow’s responses . - PBS : to look for the RBCs’ shape and any abnormalities of RBCs besides the other blood cell lines - Iron status ( Serum Iron ,TIBC, % Transferrin saturation , Iron storage ) - Blood chemistry( direct/total bilirubin,LDH and stool examination for occult blood test , etc) . PBS: Pheripheralblood smear
Lanjutan…. PendekatanDoagnostik… - Radiological examinations ( Chest X-ray, USG , MRI ) - Cardiological examinations (EKG,Treadmill, Echocardiography) Notes ! : - First confirm Anemia ( Hb , PCV , RBC ) - Classify the anemia (MCV, MCH, MCHC) - Causes of anemia
Anemia Hipokromik-Mikrositik • Setiapkondisi yang menimbulkangangguansintesisHbgambaranhipokromikmikrositik • Anemia DefisiensiBesipenyebabterseringdari anemia Hipokromik-Mikrositik • Perhatikanpenyebab lain (DD=diff diagnosis) sebelummendiagnosis Anemia def. besi, spt: - anemia akibatpenyakitkronis - Thalasemia - anemia Sideroblastik, dll
ANEMIA DEFISIENSI BESI Company Logo Definisi: Anemia yang timbulakibatkosongnyacadanganbesitubuh besiutkeritropoeisis pembentukanHb Anemia def. Fe, ditandaidgn: - anemia hipokromikmikrositik - besi serum - TIBC (Total Iron Binding Capacity) - Saturasitransferin - Feritin serum - PengecatanBesisumsumtulangnegatif - Responterhadappengobatandenganpreparat Fe
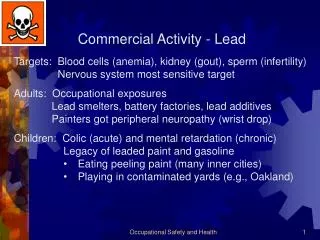
FaktorPenyebab (Etiologi) I.Keseimbangannegatif Fe (Negative Ironbalance):- Asupan Fe ↓ (inadequate diet , impaired absorption)- Fe loss ↑ (GI bleeding, excessive menstrual flow, bleeding diathesis)- ↑ demands (infancy, pregnancy, lactation)
Lanjutan….FaktorPenyebab II. Inadequate presentation to erythroid precursors:- atransferrinemia- Anti TrfRAb III. Abnormal Fe balance :- Aceruloplasminemia- Autosomal dominant hemochromatosis ( mutations in ferroportin )
Patogenesisdesifisiensi Fe • 3 pathogenetic factors:- Impaired Hb synthesis(consequence of reduced Fe supply) Transferin saturation< 16% inadequate Fe-supply to marrow → Hb contents of RBC ↓ → hypochromic & microcytosis- Generalized defect in cellular proliferation - Fe-deficient → oxidative damage to the red cell’s membrane → RBC deformability ↓ → RBC viability ↓→ RBC destruction ↑ especially in spleen → reduced RBC survival
Status besitubuh: • Serum Iron = SI • Total Iron Binding Capacity (TIBC) • % Transferrin Saturation = SI/TIBCx100% • Simpananbesi (Iron storage): - Hemosiderin →produkdegradasiferitin yang tidaklarutdalam air → mayoritastddaggregatkristal ferric oxyhydroxide, FeOOH (diHepardanSutul→ dideteksidenganbiopsi/aspirasidanpengecatanbesi (prosedurinvasif) -Ferritin → kompleksgaram Fe3+dan apoferitin yang larutdalam air, denganjumlah yang sangatkecildi serum. (dideteksidenganmetodeimunoasai)
Kandunganbesitubuh = 35-50 mg/kgBB: ±80% - Fe fungsional, sebagaiheme-Iron (65% Hb, myoglobin, enzim heme : cytochrom-C,A,A3,B, catalase , peroxidase) - Non-heme-Fe (sebagiankecil) 20% - simpananbesi / Ironstorage(ferritin, hemosiderin) hanya ± 15% padawanita 0.2%- circulating(terikatpadaTransferrin)
Iron Cycle in the body : • Fe-diet → as heme-Fe (Hb, myoglobin, enzyme-Fe), 5-35% adsorbed from animal/meat sources , adsorbed easily . → as non-heme-Fe (vegetables , legumes), 90% of diet-Fe but only 2-20% of it absorbed → depends on the iron-status and the ratio of Enhancer:Inhibitor
Enhancers (zat yang menstimulasipenyerapan (absorbsi) :Ascorbate, Cytrate, organic acids / other amino acids , by reducing Fe3+ to Fe2+. Inhibitors (zat yang menghambatabsorbsi) : Carbonate, Phytate, Tannins, Phosphate, Oxalatchelate Non-heme-Fe → unabsorbable
Bahanmakanan yang menghambatabsorbsibesi non heme (Non-heme Iron) : - Phytate (darilegumes,sayuran) - Tannin & Polyphenol (dariteh, kopi, wine, coklat) -Phosphate/phosphoproteindarikuningtelur -Minerals (Ca, Zn, Cd) - Tetracycline yang bereaksidengan Fe → menghambatabsorbsi
Siklus Fe dalamtubuh : Diet’s Iron → duodenum / proximal jejunum .Iron from gut → released into circulation , bound to transferin → distributed to body’s organ / tissues( to bone marrow as a part of heme / Hb ) → circulate inside red blood cells with blood flow
The development of IDA • Stage-1 (prelatent Fe-deficient):- progressive loss of storage-Fe- body’s Fe reserve is still sufficient to maintain both the transport and functional compartment , so RBC development is still normal .- peripheral blood picture is normal , no symptoms of anemia , but ferritin is ↓ . *IDA= Iron Deficiency Anemia
* Stage-2 (latent Fe-deficient)- Exhaustion of storage-Fe , RBC production is still normal , Ferritin ↓↓ - Circulating-Fe (SI) begin ↓ , Transf- Receptor ↑ . * Stage-3 (Fe-Deficiency Anemia)- Stadium of Iron Deficiency Anemia
PendekatanDiagnostik Anemia Defisiensi Fe 1. Anamnesis – polamenstruasi, kehamilan / persalinan, tendensiperdarahan, penyakitkronis, diet, pekerjaan, riwayatbepergian 2. Pemeriksaanfisik – sistematikdariseluruhpermukaantubuhsampaike organ dalam ( hati, limpa, kelenjargetahbening (lymphnodes)
3. Laboratorium-Hema (DL, LED, Hapusan darahtepi, Retikulosit) - Serum (SI,TIBC,Ferritin, Bilirubin) - BMA (Bone Marrow Aspiration) - Pemeriksaan Urine dantinja 4. Penunjang - Radiology (EKG, USG) - Endoscopy
Pemeriksaan Lab. Anemia def. Fe 1. CBC – confirm Anemia & find hypochromicmicrocytic picture from BSE and Red Cells Indices ( Hb, PCV ,MCV , MCH , MCHC) 2. SI – Fe2+ released from Transferrin + ferrozine (chromagen) → measured colored complex TIBC – serum + excess FeCl2 → to fill all Transferrin- binding sites → the excess Fe is fixed by Mg- carbonate → Fe-saturated Transferrin is measured with Ferrozine (= TIBC)
% SaturasiTransferrin = SI/TIBC X 100% Erythropoeisis impaired when % Tf.Sat < 15% 3. Ferritin Serum : Serum Ferritin level ~ Fe-storage Ferritin<15 ug/L → Definitive Fe-Deficient N/↑ Ferritin in IDA , if : - impaired liver function ( damaged hepatocyte), hemolysis, inflammation / infection / malignancy ( Ferritin = acute-phase protein )
4. Transferrin Serum : measured by immunodiffusionmethode Normal value : 2-4 g/L 5. Bone Marrow’s Aspirate evaluation : ( using Perls or Prussian Blue stain)
Anemia of Chronic Infection • Gejalaklinismiripdengan anemia def.Fe • Gambaran lab. hematologi = Anemia def. Fe (An.Hypo-Micro, MCV↓, MCH↓, SI↓) , tapi TIBC N/↓ and Ferritin N/↑) • Pathogenesis : Fe → storage // Transferrin Tissues / RES
Penyebabmenurunnya ‘circulating Fe’ : 1.Impairment of Fe release from macrophage in competing with lactoferrin, phagocyte’s product , even storage-Fe is still enough . 2. Inadequate EPO Respons towards anemia (effects of cytokine production by macrophage) .
Diagnosis Anemia akibatpenyakitkronis: • lab hematologi: - Anemia hipokromikmikrositik - SI ↓ , TIBC ↓/N , Ferritin N/↑ ( jikaFerritin ↓, An. Def.Fe ) - Inflamasi / infeksi (+) : CRP and LED ↑Problem: IDA with inflammation → ferritin ↑ (falsely diagnosed as ACD) ; it can be differentiated by sTfR exam (serum transferrin receptor) that ↑ in IDA but normal in ACD .