Download
1 / 31
370 likes | 894 Views
LIP AND ORAL CAVITY SQUAMOUS CELL CARCINOMAS. Guy ANDRY, M.D. Dept of Surgery Institut Jules Bordet, U.L.B. Statements 2008 on Head and Neck Cancer Frankfurt, 1 st & 2 nd February 2008. 5 Years Survival and Cause Specific Survival %. After SEER database. LIP CANCER.

E N D
LIP AND ORAL CAVITYSQUAMOUS CELL CARCINOMAS Guy ANDRY, M.D. Dept of Surgery Institut Jules Bordet, U.L.B. Statements 2008 on Head and Neck Cancer Frankfurt, 1st & 2nd February 2008
5 Years Survival and Cause Specific Survival % After SEER database
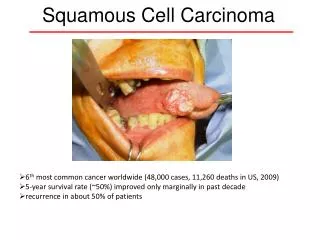
LIP CANCER • The most common primary (~ 25 % of oral cavity cancer) • ~ 12/100.000 habitants per year USA & Europe • Solar-radiation, tobacco smoking, HPV, immunosuppression
LIP CANCERSURGERY IS FIRST CHOICE • < 2/3 invasion : • full-thickness pedicled flaps (Abbe or Estlander) • > 2/3 invasion : • musculo mucosalflaps (Camille Bernard…) • free flaps • frontal flap → irradiation in debilitated PTS
LIP CANCERPROGNOSTIC FACTORS • Maximum tumor thickness (cf. Martinez-Gimeno Scoring System) • Site (upper & commissure more rapid growth and preauricular, submandibular lymph node metastases)
LIP CANCER Scoring system → probability of lymph node invasion Tumor thickness Martinez-Gimeno Scoring System T stage, Tumor thickness, microvascular, perineural invasion histologic grade of differentiation, presence of inflammatory infiltrate Group I : 0 % of lymph node invasion Group II : 21 % Group III : 50 % Group IV : 67 %
LIP CANCER • Mohs micrographic surgery has been successfully used • No tumor related deaths or metastases at 5 yrs • All PTS with recurrent disease were successfully salvaged
LIP CANCERT1 T2 Surgery if + margins + lymph nodes Adjuvant radiation Radiation if recurrence local regional External beam Brachytherapy Salvage surgery or both 98 % local control 5 yrs
LIP CANCER • There are no published randomized trials on • the use of sequential surgery + radiation • the use of chemotherapy NB : one preliminary study on super selective intraarterial chemo (CDDP based) in six PTS with T1, T2 or local recurrence by Kishi & al, Radiology 213, 1999
FLOOR OF MOUTH CANCER High risk tumors (even in early stages) • Proximity to the mandible • Adhesion or invasion (by the alveolar ridge) • Risk of radiation induced bone necrosis • No mechanical barrier in soft tissues • Blurred vision of margins, Even with high resolution MRI • Early lymph node metastases • 20 % of occult invasion in T1 • 62 % of occult invasion in T2 • Will develop second primary tumors (~ 20 % in T1 – T2) “field cancerization” effect of carcinogens
FLOOR OF MOUTH CANCER • Surgery is generally preferred for T1 T2 (primary & necks) + radiation if margins are close or involved if lymph nodes are involved (CR) if mandible is invaded if perineural or/and vascular invasion (or chemo radiation) • Role of sentinel node biopsy is under study
FLOOR OF MOUTH CANCER Neck surgery when invasion depth ≥ 5 mm level I to III unilateral for lateral tumors bilateral for anterior/midline
ORAL TONGUE CANCERT1 T2 SURGERY • Partial glossectomy (negative margins > 1 cm) → thickness, depth invasion, perineural spread, vascular invasion • Elective neck node dissection - T1 T2 T3 T4 N0 N+ 6 % 36 % 50 % 67 % After Hickx WL. & al, Am J Otolaryngol 1998 Staging is crucial in defining the postsurgical treatment ERT + CHEMO
ORAL TONGUE CANCER Role of elective neck dissection for T1 N0 ? No randomized Trial Retrospective studies remain controversial But bias in the initial treatments (various types of surgery, RT or no RT to the primary and/or to the neck)
ELECTIVE VERSUS THERAPEUTIC NECK DISSECTION IN ORAL CAVITY CANCERS Randomized trial 39 ELND36 observations T1-3 N0 49 % N+ 47 % N+ : TND 13 % CR 25 % CR DFS 5 yrs 57 % 60 % NS NB : 16 % of second primaries 45 % of deaths met caused by the original tumor After Vandenbrouck & al, Cancer 46 ; 1980
ELECTIVE VERSUS THERAPEUTIC NECK DISSECTION IN ORAL CAVITY CANCERS Randomized trial 30 hemiglossectomy + RND40 hemiglossectomy 10 N + 20 N- 23 N+ ↓ 4 contralat + 47 % N+ 57 % N+ DFS 63 % N.S 52 % (T1 : 70 % ; T2 : 60 %) (T1 : 64 % ; T2 : 46 %) After Fakih & al, Am. J. Surg. 158; 1989
ELECTIVE VERSUS THERAPEUTIC NECK DISSECTION IN ORAL CAVITY CANCERS Randomized trial : effect of tumor depth in 51 PTS 21 Hemiglossectomy + ELN 30 hemiglossectomy 9 (≥ 4 mm) 12 (< 4 mm) ↓ ↓ 6 N+ (67 %) 1 N+ (8 %) S 43 % (p < 0.01) 21 (≥ 4 mm) 9 (< 4 mm) ↓ ↓ 15 N+ (76 %) 2 N+ (22 %) S 81 % After Fakih & al, Am. J. Surg. 158; 1989
LOWER ALVEOLAR RIDGE & RETROMOLAR TRIGONE T1-2 cancers • SURGERYWide local excision with marginal mandibulectomy - close proximity to bone - infiltration into the masticator space - nodal involvement • RADIATION Adjuvant for close or positive margins for lymph node invasion OR if used as first modality
UPPER ALVEOLAR RIDGE & HARD PALATE CANCERS • SURGERY Resection of part of the palatine process → maxillectomy followed by flap reconstruction or prosthetic rehabilitation - St I (9) St II (19) St III (14)St IV(20) * CSS 75 % 46 % 36 % 11 % - neck dissection in Stage III • RADIATION : alone or used for close margins, bulky & infiltrating tumors, nodal spread After Evans & Shah, Am J Surg 1981
BUCCAL MUCOSA CANCERS • SURGERY transoral resection + check flaps + mandibular resection + maxillectomy - Neck : advocated for T2 or invasion > 5 mm, muscle St I St II St IIISt IV * 78 % 66 % 62 % 50 % N0 necks : 70 % → rec rate if no END or RT : 25 % vs 10 % (p<.05) N+ necks : 49 % (no CR : 69 % vs +CR : 24 %) + free flaps S 5yrs S 5yrs After Diaz & al, Head & Neck 2003
BUCCAL MUCOSA CANCERS (2) • RADIATION : Used primarily for cure of T 1-2 → S3yrs : St I = 85 % ; St II = 63 % * Postop advocated for high risk - margins < 2 mm • perineural invasion • lymph node involvement After Nair & al, Cancer, 1988
CONCLUSIONS (1) Prognostic factors in oral cavity SCCA • T size remains an «old timer» • Depth of invasion is more informative • as are perineural spread vascular invasion • N involvement is a state of emergency from prompt an multidisciplinary aggressive treatment
CONCLUSIONS (2) • No neck should not be a cause of debate on what is to be done in a randomized trial • Depth of invasion of the primary • Status of margins (close, involved, dysplasia,… molecular markers) • Perineural spread • Vascular invasion • Should be routinely reported and be the basis of planned treatment