Download
1 / 43
460 likes | 1.3k Views
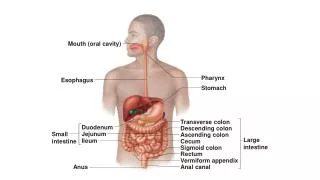
Oral Cavity and Pharynx. Hannah Lea M. David. Anatomy of the Lips and Oral Cavity. Oral Vestibule. bounded externally by the lips and cheeks and internally by the alveolar processes and teeth. Lips. Longer upper lip, shorter lower lip Connected by the Labial commisures (corners)

E N D
Oral Cavity and Pharynx Hannah Lea M. David
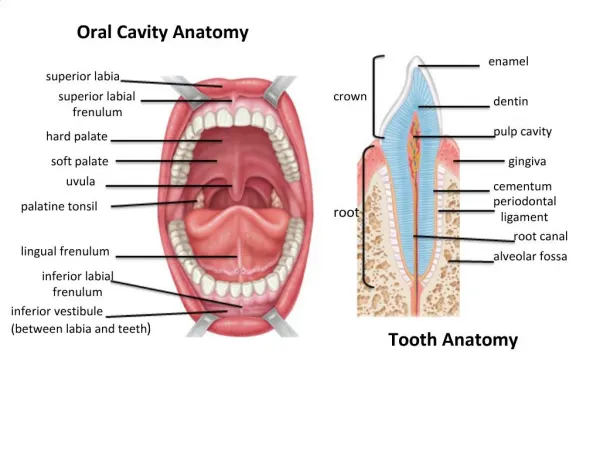
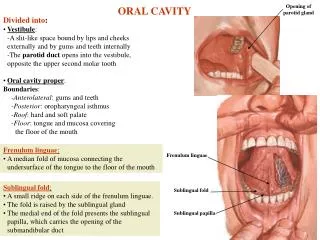
Oral Vestibule • bounded externally by the lips and cheeks and internally by the alveolar processes and teeth
Lips • Longer upper lip, shorter lower lip • Connected by the Labial commisures(corners) • Separated from the cheek by the nasolabial fold • Orbicularisoris- muscular foundation of the lips • Blood supply: Superior and inferior labial arteries (from the Facial artery) • Drained by the facial vein, which communicates with the orbital vein via the angular vein
Lips • Lymphatic drainage- submandibular and submental lymph nodes • Innervation: upper lip-infraorbital nerve; lower lip- mental nerve
Cheeks • Lateral boundaries of the oral vestibule • Buccinator- muscular framework, innervated by the facial nerve • Buccal fat pad- between the buccinator muscle and masseter • Excretory duct of the parotid gland- runs through the buccinator muscle and opens into the mucosa of the cheek opposite the upper second molar
Masticator muscles • Masseter • Temporalis muscle • Medial and Lateral pterygoid muscles • Supplied by the mandibular nerve (3rd div of the trigeminal nerve)
Teeth • Deciduous teeth, permanent teeth • 8 per maxilla/ mandible:2 incisors,1 canine, 2 premolars, 3 molars
Oral Cavity • Anterior and lateral: alveolar ridge and teeth • Superiorly: Hard and soft palate • Posteriorly: faucial isthmus
Palate • Hard palate- palatine process of the maxilla anteriorly, incisive bone, horizontal plates of the palatine bone posteriorly.\ • Soft palate- posterior; palatal muscles (tensor velipalatini, levatorvelipalatini, palatoglossus muscle) • Mucosa: contains numerous salivary glands (palatine glands) • Sensory innervation (mucosa): Greater and lesser palatine nerves • Blood supply: ascending palatine branch of the facial artery
Tongue • Mylohyoid muscle- muscular foundation • Sublingual folds and sublingual papillae- undersurface of the tongue on both sides of the frenulum • Apex, body, base • Terminal sulcus-: V-shaped groove which separates the body from the base
Tongue • Mucosa- numerous papillae (filiform, fungiform, vallate, foliate) • Blood supply (tongue and oral floor): Lingual and sublingual artery • Drainage: facial vein to the IJV • Lymphatic drainage: ipsilat and contralatsubmandibular and submental LN • Motor innervation: Hypoglossal nerve • Sensory innervation (terminal sulcus): lingual nerve, (base) glossopharyngeal and superior laryngeal nerve
Cleft Lip and Palate • Epidemiology: 1 in 500, one of the most common malformation • Classification: • Cleft lip and alveolar ridge • Cleft lip, alveolar ridge, and palate and isolated cleft palate • Symptoms: hypernasal speech (due to incomplete closure of the nasopharynx), recurrent middle ear effusions and inflammatioons, septal deviations
Pathogenesis: developmental anomaly of the embryonic head (genetic, viral infections, placental oxygen deficiency, intrauterine bleeding, exposure to ionizing radiation) • Diagnosis should include palaption of the hard palate • Tx: surgery
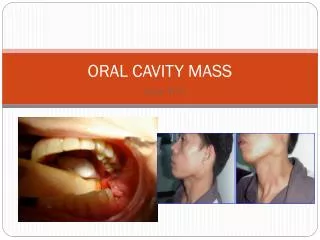
Dermoid cyst of the oral floor • Presents with submental swelling, tense bulging of the entire anterior and lateral oral floor • DDx: Dysgenetic salivary gland cyst • May also involve the tongue and mandible
Transverse facial cleft • Failure of the fusion of the maxillary and mandibular processes or failure of the buccal membrane to regress due to fusion of the myoblasts • Bilateral extension of the oral fissure • Aassociated with facial dysplasia and auricular dystropia
Inflammations of the Lips and Oral Cavity Herpes simplex Virus • Usually HSV type 1 • MOT: Contact or droplet infection • Symptoms: Primary infection- childhood, herpetic gingivostomatitis ( bullae/vesicles on the oral mucosa preceded by fever and lethargy accompanied by regional lymphadenitis) Reactivation- in response to physical exertion, fever, Uv radiation, stress, pregnancy, herpes labialism
SOP: Perioral region • Dx: History, clinical exam, Tzanck smear • Complications: secondary bacterial superinfection by Staphylococcus aureus (Herpes impetiginatus), ExudativeErythemamultiforme, Pospischill- Feyrteraphthoid, herpetic meningoenecephalitis • Tx: acyclovir
Varicella Zoster Virus • Chickenpox(primary), Zoster (reinfection) • Symptoms: Chickenpox- papulovesicular lesions esp on the head and trunk. Zoster- segmental distribution associated with neuropathic pain • Tx: acyclovir/ famciclovir
Herpangina • Causes: Group a coxsackie virus, Group B CV, Retrovirus, Echovirus • Symptoms: Fever, malaise, headache, muscle pain, bullous eruptions surrounded by red halo on the oral mucosa particularly on the anterior faucial pillars, uvula and palatine tonsils • DDx: Gingivostomatitis • Tx: Symptomatic
Recurrent aphthousstomatitis • Inflammatory shallow ulcers with slightly raised erythematous borders • Tx: Symptomatic
Oral hairy leukoplakia • Pathognomonic of HIV infection • Believed to be caused by EBV • Patchy, whitish, slightly raised lesions predominantly on the border of the tongue • Painless • Tx: topical Vit A and/or podophyllin
Oral floor Abscess • Usu. originates from the lower molars, mucosal injuries in the oral floor • Edematous expansion with a firm erythematous swelling in the submental to submandibular areas • Difficulty swallowing and speaking • High fever • May progress to ARDS or mediastinitis • Dx: US, CT to define the extent • Tx: Incision and drainage, antibiotic treatment
Candidiasis • Impaired immune sytem • Whitish, firmly adherent plaques that can be scraped from the mucosa, leaving an erythematous bleeding surface • Tx: Nystatin solution or amphotericin B lozenges
Lesions of the tongue • Hunter’s glossitis- atrophic inflammatory condition of the tongue base, acconpanying feature of PA, s/s: burning of the tongue, dry mouth, altered sense of taste, smooth shiny appearance of the tongue with partial atrophy of the filiform papillae • Fissured tongue- numerous furrows on the dorsal surface, maybe a sign of Melkersson-Rosenthal Synd • Angioedema- swelling of the face, lips, tongue and laryynx due to a pronounced vascular reaction usu in anaphylactic or anaphylactoid reactions
Geographic tongue- areas of desquamation of the filiform papillae on the dorsal surface with occ burning sensation • Black hairy tongue- hyperkeratosis of the filiform papillae due to failuure of desquamation of the cornified layers
ATROPHIC GLOSSITIS FISSURED TONGUE ANGIOEDEMA GEOGRAPHIC TONGUE BLACK HAIRY TONGUE
Benign Tumors • Epithelial or mesenchymal • Papilloma, pleomorphic adenoma, fibroma, lipoma, rhabdomyomas, leiomyomas, chondromas • Tx: surgical
Precancerous Lesions • Leukoplakia- asymptomatic, associated with denture pressure or alcohol/nicotine abuse, always investigated by biopsy, tx: complete surgical removal • Bowen’s disease- chronic inflam disease caused by intraepidermalcarcinomam
Malignant tumors (Lips) • Squamous cell carcinoma – usually affects the lower lip, associated with pipe smoking and sun exposure • Intractable ulcerations in the vermillion border of the lips or large exophytic lesions, tx: surgical removal • Basal cell Ca- involves the vermillion border of the lip only by secondary spread
Malignant Tumors (Oral cavity) • Squamous cell Ca- smoking and alcohol abuse, presents with painful swallowing, blood tinged saliva, fetid breath odor, or asymptomatic
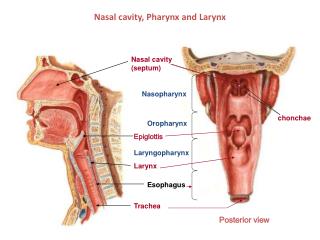
Pharynx • Tubular, fibromuscular space extending from the skull base to the inlet of the esophagus • Consists of: nasopharynx, oropharynx, hypopharynx
Nasopharynx • Highest part of the pharynx • From the bony skull bbase to an imaginary horizontal line at the level of the velum • Communicates with the nasal cavity via the choanae and middle ear via the orifice of the eustachian tube • (S) floor of the sphenoid sinus and pharyngeal roof , (P) first cervical vertebra
Oropharynx • Communicates with oral cavity via the faucial isthmus • Extends inferiorly from the lowest border of the nasopharynx to the upper margin of the epiglottis • (A) tongue base, (P) C2, C3, (L) faucial pillars
Hypopharynx • Lowest segment • From the superior border of the epiglottis to the inf border of the cricoidcatilage • (P) C3-C6, (A) back of the larynx