Download
1 / 53
550 likes | 1.3k Views
Rheumatism Infective endocarditis Chronic valvular vitium of the heart. Pathology Department Zhejiang University School of Medicine Zhu keqing 竺可青 zhukeqing@ zju.edu.cn 2013-3-18. RHEUMATISM. An immunologically mediated disease,

E N D
RheumatismInfective endocarditisChronic valvular vitium of the heart Pathology Department Zhejiang University School of Medicine Zhu keqing 竺可青 zhukeqing@zju.edu.cn 2013-3-18
RHEUMATISM An immunologically mediated disease, related to an episode of group A (β-hemolytic) streptococcal pharyngitis. Multisystem inflammatory disease, heart and joints are favored sites. Rheumatic fever, acute rheumatic carditis Repetitive attacks lead to chronic valvular deformities The pathologic feature is Aschoff bodies.
The pathogenetic sequence and key morphologic features of acute rheumatic heart disease
ESSENTIAL MORPHOLOGY (1) alteration and exudation Serous, fibrinous exudate, and leukocytes infiltration, mucoid degeneration and fibrinoid necrosis. Outcomes: Complete resolution Fibrosis Granulomas
(2) Proliferation or granulomas Hallmark:Aschoff bodies Fibrinoid necrosis, Anitschkow cells Aschoff giant cells Lymphocytes Plasma cells
Aschoff body • During acute RF, focal inflammatory lesions are found in various tissues. They are most distinctive within the heart, where they are called Aschoff bodies. • They consist of foci of swollen eosinophilic collagen surrounded by lymphocytes (primarily T cells), occasional plasma cells, and plump macrophages called Anitschkow cells (pathognomonic for RF). • These distinctive cells have abundant cytoplasm and central round-to-ovoid nuclei in which the chromatin is disposed in a central, slender, wavy ribbon (hence the designation “caterpillar cells”).形态 • Some of the larger macrophages become multinucleated to form Aschoff giant cells. 巨细胞
(3) Fibrosis Aschoff bodies spindle scar
Rheumatic endocarditis Sites: mitral and aortic valves Fibrinoid necrosis Vegetations: small, warty, along the line of closure
Precipitation of fibrin Organization, fibrosis Thickening, shortening, commissural fusion of leaflets and tendinous cord
Rheumatic myocarditis Perivascular Aschoff body
Rheumatic pericarditis Serous exudate pericardial effusion Fibrinous exudate Cor villosum Constrictive pericarditis
Rheumatic arthritis Serous inflammation Complete resolution Large joints: migratory Local signs: arthralgia Self-limited, no chronic deformity
Rheumatic arteritis Often involves small arteries, Fibrinoid necrosis Mononuclear infiltration Aschoff bodies Fibrosis Lumen narrowing
CNS changes Rheumatic arteritis, Subcortical encephalitis Minor chorea / Sydenham chorea (a neurologic disorder with involuntary purposeless, rapid movements)
ACUTE: -Inflammation -Aschoff bodies -Anitschkow cells -Pancarditis -Vegetations on chordae tendinae at leaflet junction CHRONIC: THICKENED VALVES COMMISURAL FUSION THICK, SHORT, CHORDAE TENDINAE
CLINICAL FEATURES Migratory Polyarthritis Myocarditis Subcutaneous nodules Erythema marginatum Sydenham chorea
风心小结 (肉牙肿性炎)3 stages • 变质渗出期---黏液样变/纤维素样坏死---1月 • 增生期/肉牙肿期---风湿细胞/Aschoff cell/ Aschoff body---2/3月 • 纤维化期/愈合期---4/6月
Rheumatic heart disease (小结) 1 Rheumatic endocarditis ---valvulitis---vegetations白色血栓 ---verrucous endocarditis疣状心内膜炎 ---McCallum斑 2 Rheumatic myocarditis ---Aschoff body 3 Rheumatic pericarditis---绒毛心Cor villosum---constrictive pericarditis 4 Rheumatic pancarditis
Rheumatic arthritis –游/大/无-舔关节咬心脏 • Erythema annullare 环形红斑-非特异性渗出性炎 • Subcutaneous nodules 皮下结节-风湿小体 • Rheumatic arteritis-风湿小体 • Chorea minor 小舞蹈症 • 皮质下脑炎
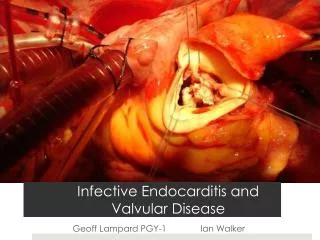
感染性心内膜炎Infective endocarditis 病原微生物直接侵袭心内膜特别是心瓣膜而引起的心内膜炎 急性感染性心内膜炎 亚急性感染性心内膜炎
急性感染性心内膜炎 病原:致病力强的化脓菌 金黄色葡萄球菌、溶血性链球菌、肺炎球菌 心瓣膜:发生在原来无病变的正常心内膜 主要累及二尖瓣、主动脉瓣 临床上:起病急,发展快,病程短,死亡率高
亚急性感染性心内膜炎 病原:致病力较小病原微生物 草绿色链球菌,肠球菌,真菌等。 心瓣膜:发生在原来有病变的心内膜 主要累及二尖瓣、主动脉瓣 菜花状或息肉状疣状赘生物: 纤维素、血小板、NC、坏死物 细菌团 血管:动脉栓塞和血管炎; 肾: 微栓塞致灶性肾小球肾炎。 临床上:病程长,数月或1年
ABE/SBE区别 • Acute endocarditis describes a destructive, tumultuous infection, frequently of a previously normal heart valve, with a highly virulent organism, that leads to death within days to weeks of more than 50% of patients despite antibiotics and surgery. • In contrast, organisms of low virulence can cause infection in a previously abnormal heart, particularly on deformed valves. In such cases, the disease may appear insidiously and, even untreated, pursue a protracted course of weeks to months (subacute endocarditis). Most patients with subacute IE recover after appropriate antibiotic therapy.
Morphology. • In both the subacute and acute forms of the disease, friable, bulky, and potentially destructive vegetations containing fibrin, inflammatory cells, and bacteria or other organisms are present on the heart valves. • Osler小结-皮下小动脉炎 • Systemic emboli may occur at any time because of the friable nature of the vegetations, and they may cause infarcts in the brain, kidneys, myocardium, and other tissues. • Because the embolic fragments contain large numbers of virulent organisms, abscesses often develop at the sites of such infarcts (septic infarcts).
Chronic valvular vitium of the heart心瓣膜病 • Vavular stenosis • Valvular insufficiency
Stenosis is the failure of a valve to open completely, thereby impeding forward flow. • Insufficiency, in contrast, results from failure of a valve to close completely, thereby allowing reversed flow.
Aortic stenosis: calcification of anatomically normal and congenitally bicuspid aortic valves. • Aortic insufficiency: dilation of the ascending aorta, related to hypertension and aging. • Mitral stenosis: rheumatic heart disease. • Mitral insufficiency: myxomatous degeneration (mitral valve prolapse).
70% of all VHD AS Calcification of a deformed valve “Senile” calcific AS Rheum, Heart Dis. MS Rheumatic Heart Disease
二尖瓣狭窄X线检查 左心房增大 胸骨左缘第3肋间心浊音界增大,使心腰消失,如梨形,称二尖瓣型心(三大一小—梨型心) 风心病二狭,瓣口面积1.2cm2
主动脉瓣关闭不全X线检查 左心室增大向左下增大,心腰加深,似靴形:见于主动脉瓣关闭不全 男,36岁,风心病,主动脉瓣关闭不全 左心室80mm
AORTIC STENOSIS 2X gradient pressure LVH (but no hypertension), ischemia Cardiac decompensation, angina, CHF 50% die in 5 years if angina present 50% die in 2 years if CHF present
MITRAL ANNULAR CALCIFICATION Calcification of the mitral “skeleton” Usually NO dysfunction Regurgitation usually, but Stenosis possible F>>M
REGURGITATIONS AR Rheumatic Infectious Aortic dilatations Syphilis Rheumatoid Arthritis Marfan MR MVP Infectious Fen-Phen Papillary muscles, chordae tendinae Calcification of mitral ring (annulus)
Mitral Valve Prolapse (MVP) MYXOMATOUS degeneration of the mitral valve Associated with connective tissue disorders “Floppy” valve 3% incidence, F>>M Easily seen on echocardiogram
MVP: CLINICAL FEATURES Usually asymptomatic Mid-systolic “click” Holosystolic murmur if regurg. present Occasional chest pain, dyspnea 97% NO untoward effects 3% Infective endocarditis, mitral insufficiency, arrythmias, sudden death