Download
1 / 17
180 likes | 768 Views
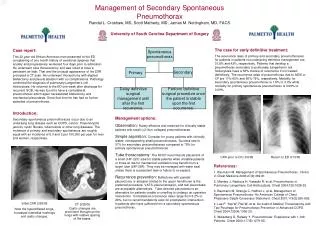
VATS Treatment of Spontaneous Pneumothorax. William R. Mayfield, MD, FACS WellStar Thoracic Surgery March 2009. Etiology Bleb rupture Primary Secondary . Consensus Statement . Management of Spontaneous Pneumothorax * An American College of Chest Physicians Delphi Consensus Statement

E N D
VATS Treatment of Spontaneous Pneumothorax William R. Mayfield, MD, FACS WellStar Thoracic Surgery March 2009
Etiology • Bleb rupture • Primary • Secondary
Consensus Statement Management of Spontaneous Pneumothorax* An American College of Chest Physicians Delphi Consensus Statement MICHAEL H. BAUMANN, MD, FCCP, et al FOR THE ACCP PNEUMOTHORAX CONSENSUS GROUP† CHEST FEBRUARY 2001 VOL. 119 NO. 2 590-602
Primary Spontaneous Pneumothorax • Clinically Stable • Small Pneumothorax • Observe in ER for 3-6 hrs • Repeat CXR • If no progression: discharge home • If distant from ER, or compliance unreliable, then admit
Primary Spontaneous Pneumothorax • Clinically stable • Large pneumothorax • Small bore catheter, 14 fr to 22 fr • Water seal • Suction if no re-expansion • Remove chest tube when no air leak • Discharge with one-way valve if unwilling to be admitted
Primary Spontaneous Pneumothorax • Unstable • Large pneumothorax • Chest tube 16 – 22 fr if small leak anticipated • Chest tube 24 – 28 fr if large leak anticipated, or positive pressure ventilation anticipated • Water seal • Suction if lung fails to expand • Remove tube when no leak and lung expanded
Persistent Air Leak • Greater than 4 days • Thoracoscopy • Closure of leak • Pleurodesis • Bedside pleurodesis • Only if surgery contra-indicated or patient refuses surgery • Doxycycline or talc slurry
Pneumothorax Recurrence Prevention • First pneumothorax 15% of panel • Second pneumothorax 85% of panel • Decision modified by desire to fly or scuba • Thoracoscopy is treatment of choice • 95 – 100% success • Bullectomy • Parietal pleural abrasion of upper 50% • Pleurectomy is acceptable • Talc: no consensus • Bedside pleurodesis for high risk patients • 78 – 91% success
Primary Spontaneous Pneumothorax • CT scanning • No consensus for first time pneumothorax • No consensus for second time pneumothorax, persistent air leak, or planned surgery
Position • Lateral decubitus, flexed • Incisions • Two incision technique: 3rd and 6th interspace
Video • 5 mm chip on a stick (Olympus) • Endo GIA • Green load • Duet in bullous disease
Case Report • 87 yo male • Metastatic angio-sarcoma • Multiple pulmonary blebs after chemotherapy • Recurrent left pneumothorax • Failed bedside talc pleurodesis • prior admission
Conclusions • There is consensus on treatment of spontaneous pneumothorax • It is acceptable to operate on first time pneumothorax • Thoracoscopy is the preferred method • Pleurodesis by abrasion, pleurectomy, or (sometimes) talc is acceptable