Download
1 / 59
640 likes | 1.56k Views
Achilles: Hero of the Iliad. Led Greeks to conquer TroyKilled by arrow shot to heelHippocrates ? ? this tendon if bruised or cut, causes the most acute fevers, induces choking, deranges the mind and at length brings death."Strongest tendon in the human body. Achilles Tendon. Formed by tendinous

E N D
1. Achilles Tendon Ruptures Steven B. Weinfeld, MD
Associate Professor of Orthopaedic Surgery
Chief; Foot and Ankle Service
Mount Sinai Medical Center, NY
2. Achilles: Hero of the Iliad Led Greeks to conquer Troy
Killed by arrow shot to heel
Hippocrates � � this tendon if bruised or cut, causes the most acute fevers, induces choking, deranges the mind and at length brings death.�
Strongest tendon in the human body
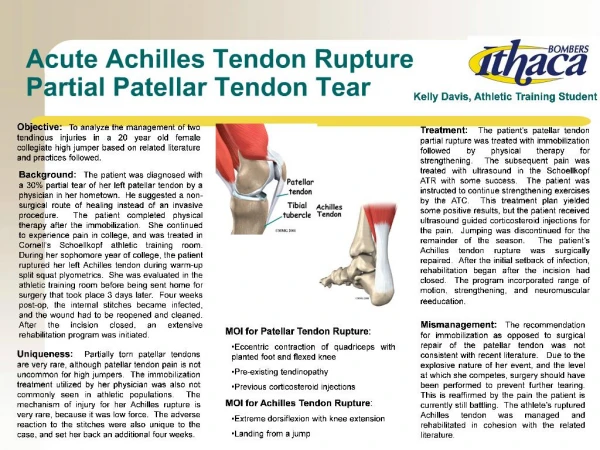
3. Achilles Tendon Formed by tendinous portion of gastrocnemius and soleus
Plantaris lies medial and is distinct tendon
Achilles progresses from round to flat as it travels distally to insert on calcaneal tuberosity
Fibers of tendon rotate 90 degrees distally with medial fibers terminating posteriorly
4. Biochemistry Collagen comprises 70% of tendon
95% type I
Small amount of elastin
Collagen organized into fascicles surrounded by epitenon
Ruptured tendon contains significant type III collagen
5. Blood Supply Musculotendinous junction
Surrounding connective tissue (paratenon)
Bone-tendon junction
Poor vascularization in midportion of tendon
Ref: Schmidt-Rolfing, Int. Orthop., 1992
6. Biomechanics Peak force of 2233 newtons within achilles in vivo- Fukashiro 1995
Force builds just before heel strike, then released
Force builds again and peaks at the end of push off
Injury can be produced by asynchronous contraction of triceps surae
7. Biomechanics � continued At rest, tendon has wavy configuration
Tensile stress causes loss of waves
Collagen fibers respond linearly to stresses
Can return to original configuration with physiologic loads
If force greater than physiologic, cross links damaged and ultimately macroscopic rupture occurs � Kannus 1997
8. Epidemiology Incidence 18 per 100,000 - Finland
Most ruptures occur during sports (Badminton)
More common in males in third and fourth decade of life
Blood type O?
9. Etiology Inflammatory and autoimmune conditions
Collagen disorders
Infectious disease
Neurologic conditions
Blood flow to tendon decreases with age
Area prone to rupture relatively hypovascular
10. Etiology � continued Histologic evidence of collagen degeneration in all studies of patients with rupture
Collagen degeneration occurs prior to rupture
Alternating exercise with inactivity
Accumulation of trauma leads to degeneration
Corticosteroids � injection into rabbit tendons showed necrosis and delayed healing. Several studies showed collagen damage with injected steroids
Oral steroids also implicated
11. Fluoroquinolones and Tendon Rupture Ciprofloxacin
Direct deleterious effect on tenocytes
Decreased transcription of Decorin which may modify architecture of tendon and alter mechanical properties
Bernard-Beaubois 1998
12. Mechanism of Rupture Pushing off foot while extending knee- 53%
Jumping in basketball
Volleyball
Sudden dorsiflexion of ankle- 17%
Fall down steps or into hole
Violent dorsiflexion of plantar flexed foot- 10%
Fall from height
13. Histology of Rupture Degeneration of tendon
Patches of mucoid degeneration
Marked inflammatory reaction
Hypertrophy of tunica media of large peritendinous vessels
All based on biopsy at time of surgical repair
14. Clinical Presentation Sudden pain in affected limb
Report being �struck in back of leg�
Edema and bruising
Palpable gap in tendon
+ Thompson test- 1962
Frequently missed!!
17. Imaging Radiographs- usually not helpful unless avulsion of calcaneus
Ultrasound � used to assess gap in tendon and apposition of torn ends of tendon
Helpful with nonoperative tx
MRI � useful in partial tears and tendinosis
18. Achilles Tendon Healing Rabbit model � Thermann et al Germany
Foot and Ankle July 2002
Nonoperative vs. operative
No difference within first week
Nonop tx showed aligned fibroblasts after 1 week
At 12 weeks, nonop=op tx
High levels of type III collagen in healing tissue of ruptured tendons
19. Achilles Tendon Healing Balb-C mice with ruptured achilles treated either with mobilization or immobilization
More rapid restoration of load to failure in mobilized group
112 days mobilized group regained original tendon stiffness
Mobilization lead to increased inflammatory cells at rupture site.
Palmes et al J of Orthopaedic Research 2002
20. Nonoperative Treatment Cast immobilization 6-8 weeks
Functional brace
Use ultrasound to ensure tendon apposition
Higher rerupture rate vs. operative repair
Fewer overall complications
21. Surgical Treatment First advocated by Pare 1575
1-2% deep infection rate
Rerupture rate 2-8%
Pajala et al JBJS 2002
409 patients, 5.6% rerupture rate
2.2% deep infection- Finlan
22. Surgical Repair vs. Casting 7.7% rerupture rate with cast vs. 3% with surgery
AOFAS scores similar at 3.5 years post rupture.
Greater calf atrophy with cast
Fewer overall complications with nonoperative tx
Beskin et al Foot/Ankle December 2001
28. Complications of Surgical Treatment Wound necrosis
Wound infection
Sural nerve injury
DVT and PE
Rerupture 2-5%
32.
34. Percutaneous Achilles Repair Developed by Ma and Griffith 1977
6 small incisions to pass sutures
Faster return to normal strength than cast
Sural nerve entrapment
Higher rerupture rate vs. open repair
35. Percutaneous vs. Open Repair Percutaneous
6.4% rerupture rate
Open repair
2.7% rerupture
Percutaneous does not reestablish length
Injury to sural nerve
Fewer wound complications with percutaneous tx
JBJS Br 1999
36. Chronic Ruptures Use V-Y advancement if gap < 4cm
Central turn down for larger gaps > 4cm
Augmentation with FHL tendon
Allografts?
51. Achilles Tendonitis Thickening and swelling of tendon
May occur at insertion or midsubstance
Often associated with tight gastroc
Insidious onset
52. Achilles Tendonitis - Treatment Immobilization
Physical therapy
Heel lift
NSAIDS
PRP injection
NO CORTISONE!
56. Operative vs. Nonoperative Treatment Willits et al, JBJS Dec 2010
144 patients with achilles rupture
Randomized to operative and nonoperative
Fewer complications in nonoperative group
Functional outcome no statistical difference
57. Summary Functional outcome better with surgery and early motion
Fewer complications with nonsurgical tx
Rerupture rate
Surgery 2%
Cast 8-10%
Future
Functional bracing
Percutaneous repair
58. Postoperative Protocol Non weight bearing x 4 weeks
Cam walker brace x 6 weeks
Active ROM exercises only
No passive stretching for 8 weeks
�� heel lift x 6 months
59. That�s All Folks!