Download
1 / 29
330 likes | 1.03k Views
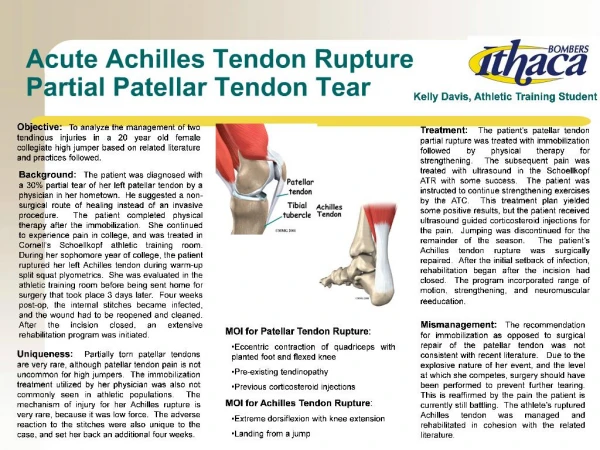
Achilles Tendon Disorders. Daniel Penello Foot & Ankle Rounds. Anatomy. Largest tendon in the body Origin from gastrocnemius and soleus muscles Insertion on calcaneal tuberosity. Anatomy. Lacks a true synovial sheath Paratenon has visceral and parietal layers

E N D
Achilles Tendon Disorders Daniel Penello Foot & Ankle Rounds
Anatomy • Largest tendon in the body • Origin from gastrocnemius and soleus muscles • Insertion on calcaneal tuberosity
Anatomy • Lacks a true synovial sheath • Paratenon has visceral and parietal layers • Allows for 1.5cm of tendon glide
Anatomy • Paratenon • Anterior – richly vascularized • The remainder – multiple thin membranes
Anatomy • Blood supply • Musculotendinous junction • Osseous insertion on calcaneus • Multiple mesotenal vessels on anterior surface of paratenon (in adipose) • Transverse vincula • Fewest @ 2 to 6 cm proximal to osseous insertion
Physiology • Remarkable response to stress • Exercise induces tendon diameter increase • Inactivity or immobilization causes rapid atrophy • Age-related decreases in cell density, collagen fibril diameter and density • Older athletes have higher injury susceptibility
Biomechanics • Gastrocnemius-soleus-Achilles complex • Spans 3 joints • Flex knee • Plantar flex tibiotalar joint • Supinate subtalar joint • Up to 10 times body weight through tendon when running
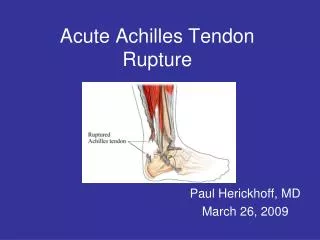
Achilles Tendon Rupture • Pathophysiology • Repetitive microtrauma in a relatively hypovascular area. • Reparative process unable to keep up • May be on the background of a degenerative tendon
Achilles Tendon Rupture: Textbook Facts • Antecedent tendinitis/tendinosis in 15% • 75% of sports-related ruptures happen in patients between 30-40 years of age. • Most ruptures occur in watershed area 4cm proximal to the calcaneal insertion.
Achilles Tendon Rupture • History • Feels like being kicked in the leg • Case reports of fluoroquinolone use, steroid injections • Mechanism • Eccentric loading (running backwards in tennis) • Sudden unexpected dorsiflexion of ankle • (Direct blow or laceration)
Physical Exam • Prone patient with feet over edge of bed • Palpation of entire length of muscle-tendon unit during active and passive ROM • Compare tendon width to other side • Note tenderness, crepitation, warmth, swelling, nodularity, palpable defects
Achilles Tendon Rupture • Physical • Partial • Localized tenderness +/- nodularity • Complete • Defect • Cannot heel raise • Positive Thompson test
Achilles Tendon Rupture • Diagnostic Pitfalls • 23% missed by Primary Physician (Inglis & Sculco) • Tendon defect can be masked by hematoma • Plantar-flexion power of extrinsic foot flexors retained • Thompson test can produce a false-negative if accessory ankle flexors also squeezed
Imaging • Ultrasound • Inexpensive, fast, reproducable, dynamic examination possible • Operator dependent • Best to measure thickness and gap • Good screening test for complete rupture
Imaging • MRI • Expensive, not dynamic • Better at detecting partial ruptures and staging degenerative changes, (monitor healing)
Management Goals • Restore musculotendinous length and tension. • Optimize gastro-soleous strength and function • Avoid ankle stiffness
Conservative Management CAM Walker or cast with plantarflexion q 2 wks Cast in Plantarflexion 2 wks 4 weeks Allow progressive weight-bearing in removable cast Start physio for ROM exercises When WBAT and foot is plantigrade 2- 4 weeks Start a strengthening program Remove cast and walk with shoe lift. Start with 2cm x 1 month, then 1cm x1 month then D/C
Surgical Management • Preserve anterior paratenon blood supply • Beware of sural nerve • Debride and approximate tendon ends • Use 2-4 stranded locked suture technique • May augment with absorbable suture • Close paratenon separately
Surgical Management • Bunnell Suture • Modified Kessler • Many techniques available
Surgical Management : Post– op Care • Assess strength of repair, tension and ROM intra-op. • Apply cast with ankle in the least amount of plantarflexion that can be safely attained. • Patient returns to fracture clinic 2 weeks post-op.
Post- Op Care Remove sutures, apply a walking cast with heel lift Cast applied in OR 2 wks Touch WB 2 weeks Allow progressive weight-bearing in removable cast Start physio for ROM exercises. No active plantarflexion When WBAT and foot is plantigrade 2- 4 weeks Start a strengthening program Remove cast and walk with a 1cm shoe lift x 1 month then D/C.
Surgical Management:Post-op Care Early functional treatment versus early immobilization in tension of the musculotendinous unit after Achilles rupture repair: a prospective, randomized, clinical study. Kangas J et al. J Trauma. 2003 Jun;54(6):1171-80; discussion 1180-1. 50 pts had repair of Achilles rupture 25 25 Casted in neutral x 6 weeks. WBAT at 3 weeks Immediate active ROM from PF to neutral. WBAT at 3 wk Two re-ruptures One deep infection Same satisfaction Better calf strength only for first 3 months. One re-rupture
Conservative vs Surgical Acute rupture of tendon Achillis. A prospective randomised study of comparison between surgical and non-surgical treatment.Moller M, et al. J Bone Joint Surg Br. 2001 Aug;83(5):863-8 112 patients Casted x 8 wks Surgery + Early functional rehab in brace 21 % re-rupture 1.7% re-rupture 5% infection 2% Sural nerve inj. No difference in functional outcome
Risk of Re-Rupture • Surgery = 68% risk reduction for re-rupture