Download
1 / 46
460 likes | 897 Views
Testis Cancer. Christopher Saigal MD MPH Associate Professor UCLA Dept of Urology. Differential Burden of illness Screening Diagnosis Treatment Patient centered outcomes. Differential. Differential of a scrotal mass:

E N D
Testis Cancer Christopher Saigal MD MPH Associate Professor UCLA Dept of Urology
Differential • Burden of illness • Screening • Diagnosis • Treatment • Patient centered outcomes
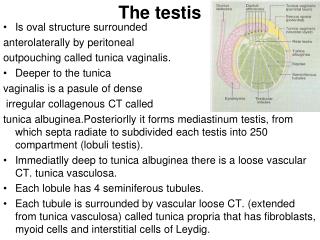
Differential Differential of a scrotal mass: History: Time course, associated pain, constitutional symptoms, exacerbating factors, etc Past medical history: undescended testis, maternal DES exposure, h/o contralateral tumor
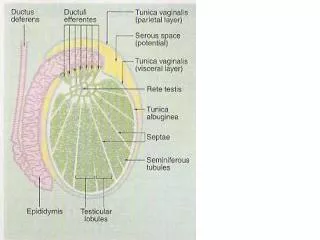
Evaluation of Scrotal Mass • Physical exam: Vitals Pain, redness, heat, reducibility, orientation of testis Phren’s sign Transillumination Cremasteric reflex • UA, urine culture • Ultrasound
Differential: Epididymo-orchitis • Epididymitis is most common • Usually an ascending infection thru vas deferens • Age predicts causative organism >35 yrs: coliform bacteria 12-35 yrs: chlamydia, gonorrhea <12: coliform, ?viruses
Differential: Hernia Reducible or incarcerated Usually does not transilluminate Swells with valsalva
Differential: benign testicular lesions Very rare. Ultrasound may be suggestive • epidermoid cysts • fibromas • fibroadenomas • adenomatoid tumors • lipomas
Differential: testis tumor • Physical exam ?gynecomastia (found in 5%) adenopathy abdominal mass
Burden of Illness • Incidence rose from 3.5 to 6.5/100,000 over 30 years • About 6,000 cases/yr • Survival is > 90% • For all males, lifetime probability of dying of testes cancer is 0.02% SEER
Testicular Cancer: Is Screening Accurate Can screen via: Testicular self exam: Low specificity: about 8% of men with a “lump” found to have a tumor Buetow J, Med Screen. 1996 Testicular ultrasound: Highly sensitive and specific
Does Screening Improve Outcomes? • US Preventative Services Task Force 4/2004 Review • No evidence of decreased mortality • 5 yr survival is >90% without screening • Risk of false positives with TSE • Cannot recommend screening
Diagnosis Ultrasound is highly specific (hypoechoic lesion), but diagnosis is made at radical orchiectomy Microlithiasis- not a risk factor Biopsy contraindicated
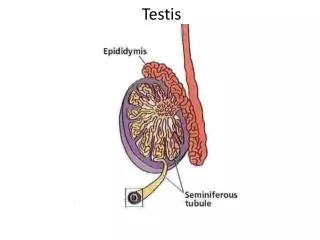
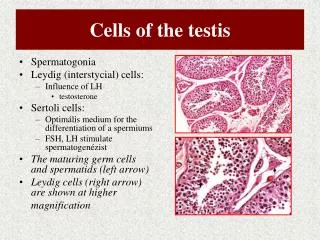
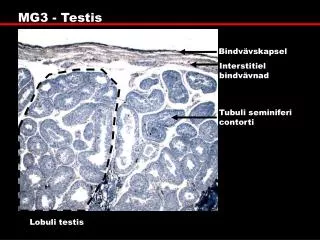
Histologic types Germ cell tumors: Seminoma versus Non seminomatous germ cell tumors (NSGCT) Non-germ cell tumors (rare, <5%) Leydig cell tumors (precocious puberty) Sertoli cell tumors Mixed sex chord-stromal tumors
NSGCT • Choriocarcinoma (elevated b-Hcg) • Embryonal cell • Teratoma (mature and immature) • Yolk sac (elevated AFP)
Seminoma • Rarely make hcg • Generally favorable prognosis when seen in older men
Tumor markers • AFP levels are elevated 50%-70% NSGCT • hCG levels are elevated in 40%-60%. • AFP has a half-life of 5-7 days • hCG has a half-life of 36 hours. • Important to follow response after orchiectomy • LDH is non-specific measure of tumor burden
Treatment • Staging CT scan miss microscopic disease in 1 in 3 to 1 in 5 men • % embryonal cell, LV invasion, T stage can be predictive or RP disease • Dilemma: overtreat or undertreat?
Treatment Seminoma Stage IA and B: radiation therapy vs surveillance (? Chemo) NSGCT Stage IA retroperitoneal lymph node dissection vs surveillance Stage IB retroperitoneal lymph node dissection vs surveillance vs chemotherapy Higher stages-chemo, f/b surgery as needed
Endocrine issues • Higher proportion of oligospermic men • Sperm banking recommended before adjuvant therapy • Treatment can damage testis, decrease T levels • Leydig cell tumors, some that produce B-hcg can cause gynecomastia
chemotherapy • Usually 2 cycles of BEP • Well tolerated • ? Late effects • Effects on fertility
Surveillance NCCN guidelines • CT q 2-3 months for first year or two • Then q4, q6 • Labs, CXR q month for year one, then q 2 months, etc • Issues are compliance, anxiety
FOLLOW UP YEAR N* COMPLIANCE† N* COMPLIANCE† Abdominal Imaging Abdominal Imaging Chest Imaging Chest Imaging Labs / Tumor Markers Labs / Tumor Markers 100% ≥50% 100% 0% ≥50% 100% 0% ≥50% 100% 0% ≥50% 100% 0% ≥50% 100% 0% ≥50% 0% Surveillance For Seminoma 1 397 1 39.5% 397 14.9% 39.5% 22.4% 14.9% 56.7% 22.4% 17.4% 56.7% 25.9% 17.4% 41.8% 25.9% 10.3% 41.8% 27.5% 10.3% 27.5% 2 227 2 15.9% 227 17.2% 15.9% 39.6% 17.2% 40.1% 39.6% 20.3% 40.1% 39.6% 20.3% 30.4% 39.6% 11.9% 30.4% 34.8% 11.9% 34.8% 3 110 3 3.6% 110 19.1% 3.6% 45.5% 19.1% 21.8% 45.5% 30.9% 21.8% 47.3% 30.9% 25.5% 47.3% 17.3% 25.5% 39.1% 17.3% 39.1% 4 61 4 6.6% 61 31.1% 6.6% 62.3% 31.1% 42.6% 62.3% NA 42.6% 57.4% NA 27.9% 57.4% 23.0% 27.9% 49.2% 23.0% 49.2% 5 19 5 0% 19 36.8% 0% 63.2% 36.8% 42.1% 63.2% NA 42.1% 57.9% NA 21.1% 57.9% 21.1% 21.1% 57.9% 21.1% 57.9% Surveillance For NSGCT 1 397 23.7% 30.7% 22.4% 12.3% 28.5% 25.9% 21.4% 20.4% 27.5% 2 227 5.3% 27.8% 39.6% 3.1% 20.3% 39.6% 13.2% 17.2% 34.8% 3 110 3.6% 19.1% 45.5% 3.6% 18.2% 47.3% 13.6% 29.1% 39.1% 4 61 6.6% 31.1% 62.3% 3.3% 8.2% 57.4% 11.5% 16.4% 49.2% 5 19 36.8% NA 63.2% 10.5% 31.6% 57.9% 21.1% 21.1% 57.9% Post - RPLND 1 96 68.8% 22.9% 8.3% 60.4% 33.3% 0% 57.3% 16.7% 14.6% 2 61 62.3% NA 37.7% 27.9% 37.7% 14.8% 23.0% 29.5% 26.2% 3 28 60.7% NA 39.3% 17.9% 28.6% 28.6% 25.0% 14.3% 32.1% 4 14 50.0% NA 50.0% 14.3% 28.6% 14.3% 14.3% 21.4% 42.9% 5 7 28.6% NA 71.4% 0% 14.3% 85.7% 28.6% 42.9% 28.6% Post - XRT 1 541 19.8% 30.1% 11.8% 28.8% 27.2% 15.3% 43.6% 16.5% 23.3% 2 309 19.7% 38.5% 41.7% 32.7% 36.2% 31.1% 41.1% 27.2% 31.7% 3 155 45.2% NA 54.8% 59.4% NA 40.6% 59.4% NA 40.6% 4 76 35.5% NA 64.5% 51.3% NA 48.7% 57.9% NA 42.1% 5 23 13.0% NA 87.0% 30.4% NA 69.6% 60.9% NA 39.1% Quality of Surveillance for Stage I Testis Cancer in the Community Stage I Testis Cancer Compliance With Surveillance Follow Up Guidelines for Seminoma • 401, 96, and 541 patients received surveillance, RPLND and XRT, respectively. • Mean follow up was 23, 24 mo, and 23 months, respectively. • 100% of surveillance patients had at least one follow up test in the first year, but 8-16% of patients had no follow tests of any kind in years 2-5. • Compliance with recommended follow up was generally poor. • Compliance with follow up was higher in RPLND patients.
Quality of Surveillance for Stage I Testis Cancer in the Community • The use of surveillance for testis cancer is widely accepted in the community. • Compliance rates with recommended follow up care are poor . • Compliance among RPLND patients appear to be superior, possibly due to greater selection for motivated patients. • Surveillance protocols developed at referral centers are not being followed in the community; further work is needed to understand the impact of this apparent quality of care problem on oncologic outcomes in men treated in the community with surveillance protocols.
Testicular Cancer outcomes 5 year survival for stage I is >95% Focus is on reducing treatment side effects (e.g. retrograde ejaculation) Concern over late effects of treatment
California Cancer Registry study • Decision Regret Scale • Short Form - 12 • Hospital Anxiety and Depression Scale • Locus of Control Scale • Tolerance of Ambiguity Scale • Questions about influencers, satisfaction
PHYSICIAN CONSULTATIONS Urologist Oncologist RadOnc Seminoma Surveillance 1.2 0.4 1.1 XRT 1.3 0.5 0.9 NSGCT Surveillance 1.5 0.7 Chemo 1.0 1.2 RPLND 2.2 1.2
DECISION INFLUENCE Urologist Oncologist RadOnc Seminoma Surveillance 4.3 4.7 4.8 XRT 4.5 4.5 4.6 NSGCT Surveillance 4.5 4.9 Chemo 4.5 4.6 RPLND 4.4 3.7 Family, friends, cost, time missed from work, internet mainly 2-3
COUNSELING ADEQUACY Urologist Oncologist RadOnc Seminoma Surveillance 4.3 4.3 4.8 XRT 4.2 4.4 4.4 NSGCT Surveillance 4.2 4.9 Chemo 4.0 4.4 RPLND 4.4 3.7
PATIENT SATISFACTION Urologist Oncologist RadOnc Seminoma Surveillance 4.9 4.5 4.5 XRT 4.4 4.4 4.4 NSGCT Surveillance 4.6 4.8 Chemo 4.3 4.0 RPLND 4.2 4.0
DECISION REGRET SCALE DRS Score Seminoma XRT 14.5 NSGCT Surveillance 15.5 Chemo 30.8 RPLND 20.4
OTHER INSTRUMENTS • Short Form - 12: • Physical component scores: • Similar between treatment groups • Higher than age matched population means • Mental component scores • Similar between treatment groups • Similar to age matched population means. • Tolerance of Ambiguity Scale: • Similar between treatment groups
OTHER INSTRUMENTS • Hospital Anxiety and Depression Score: • Similar between treatment groups • All groups scored in the borderline abnormal range • Locus of Control Scale: • Influence of chance < internal < powerful others. • Adjuvant therapy patients influenced more by powerful others. • RPLND patients have stronger internal LCS than other treatment groups.
CONCLUSIONS • Influence of the MD is important • RadOncs and Oncologists may doing better job of pt counseling • Pts generally tolerate surveillance and treatments well and do not regret their choice
CONCLUSIONS • Despite borderline anxiety and depression scores, pts do not show mental QOL impairment compared with population – including recurrences • Surveillance pts do not experience more anxiety or depression
CONCLUSIONS • Clinical outcome may not be the ultimate determinate of patient satisfaction • Prospective studies need to be done to evaluate true effect of surveillance vs treatments and the effects of clinical recurrence on pt satisfaction and QOL
Surveillance and Treatment Expenditures of Stage I Testis Cancer Stage I Testis Cancer Follow Up Expenditures
Surveillance and Treatment Expenditures of Stage I Testis Cancer • Long-term expenditures for stage I testis cancer are lowest after XRT. • Expenditures for surveillance were less than that for RPLND, but greater than that for XRT, even though no active treatment occurs. • Follow-up tests do not account for the bulk of expenditures - surveillance patients are incurring more expenses related to physician and hospital services, including treatment for recurrences. • Actual expenditures may vary from projected models due to high rates of non-compliance with follow up protocols. • Prospective studies on the clinical and economic impact s of surveillance noncompliance within the community need to be done.