Download
1 / 1
10 likes | 133 Views
Imaging of Focal Nodular Hyperplasia: A Review 1 Joseph R. Grajo, M.D., 2 Richard G. Barr, M.D, Ph.D., 3 Peter L. Apicella, M.D., 4 Rajendra P. Kedar, M.D. 1 University of South Florida, Department of Radiology, Tampa, FL 2 Southwoods Radiology Consultants, Youngstown, OH

E N D
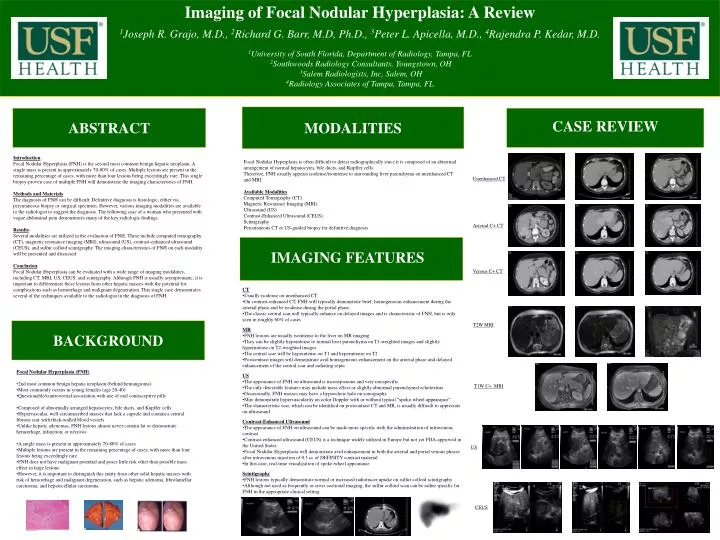
Imaging of Focal Nodular Hyperplasia: A Review 1Joseph R. Grajo, M.D., 2Richard G. Barr, M.D, Ph.D., 3Peter L. Apicella, M.D., 4Rajendra P. Kedar, M.D. 1University of South Florida, Department of Radiology, Tampa, FL 2Southwoods Radiology Consultants, Youngstown, OH 3Salem Radiologists, Inc, Salem, OH 4Radiology Associates of Tampa, Tampa, FL MODALITIES ABSTRACT CASE REVIEW Introduction: Focal Nodular Hyperplasia (FNH) is the second most common benign hepatic neoplasm. A single mass is present in approximately 70-80% of cases. Multiple lesions are present in the remaining percentage of cases, with more than four lesions being exceedingly rare. This single biopsy-proven case of multiple FNH will demonstrate the imaging characteristics of FNH. Methods and Materials: The diagnosis of FNH can be difficult. Definitive diagnosis is histologic, either via percutaneous biopsy or surgical specimen. However, various imaging modalities are available to the radiologist to suggest the diagnosis. The following case of a woman who presented with vague abdominal pain demonstrates many of the key radiologic findings. Results: Several modalities are utilized in the evaluation of FNH. These include computed tomography (CT), magnetic resonance imaging (MRI), ultrasound (US), contrast-enhanced ultrasound (CEUS), and sulfur colloid scintigraphy. The imaging characteristics of FNH on each modality will be presented and discussed. Conclusion: Focal Nodular Hyperplasia can be evaluated with a wide range of imaging modalities, including CT, MRI, US, CEUS, and scintigraphy. Although FNH is usually asymptomatic, it is important to differentiate these lesions from other hepatic masses with the potential for complications such as hemorrhage and malignant degeneration. This single case demonstrates several of the techniques available to the radiologist in the diagnosis of FNH. • Focal Nodular Hyperplasia is often difficult to detect radiographically since it is composed of an abnormal arrangement of normal hepatocytes, bile ducts, and Kupffer cells. • Therefore, FNH usually appears isodense/isointense to surrounding liver parenchyma on unenhanced CT and MRI. • Available Modalities • Computed Tomography (CT) • Magnetic Resonance Imaging (MRI) • Ultrasound (US) • Contrast-Enhanced Ultrasound (CEUS) • Scintigraphy • Percutaneous CT or US-guided biopsy for definitive diagnosis Unenhanced CT Arterial C+ CT IMAGING FEATURES Venous C+ CT • CT • Usually isodense on unenhanced CT • On contrast-enhanced CT, FNH will typically demonstrate brief, homogeneous enhancement during the arterial phase and be isodense during the portal phase • The classic central scar will typically enhance on delayed images and is characteristic of FNH, but is only seen in roughly 60% of cases • MR • FNH lesions are usually isointense to the liver on MR imaging • They can be slightly hypointense to normal liver parenchyma on T1-weighted images and slightly hyperintense on T2-weighted images • The central scar will be hypointense on T1 and hyperintense on T2 • Postcontrast images will demonstrate avid homogeneous enhancement on the arterial phase and delayed enhancement of the central scar and radiating septa • US • The appearance of FNH on ultrasound is inconspicuous and very nonspecific • The only detectable features may include mass effect or slightly abnormal parenchymal echotexture • Occasionally, FNH masses may have a hypoechoic halo on sonography • May demonstrate hypervascularity on color Doppler with or without typical “spoke-wheel appearance” • The characteristic scar, which can be identified on postcontrast CT and MR, is usually difficult to appreciate on ultrasound • Contrast-Enhanced Ultrasound • The appearance of FNH on ultrasound can be made more specific with the administration of intravenous contrast • Contrast-enhanced ultrasound (CEUS) is a technique widely utilized in Europe but not yet FDA-approved in the United States • Focal Nodular Hyperplasia will demonstrate avid enhancement in both the arterial and portal venous phases after intravenous injection of 0.3 cc of DEFINITY contrast material • In this case, real-time visualization of spoke-wheel appearance • Scintigraphy • FNH lesions typically demonstrate normal or increased radiotracer uptake on sulfur colloid scintigraphy • Although not used as frequently as cross-sectional imaging, the sulfur colloid scan can be rather specific for FNH in the appropriate clinical setting BACKGROUND T2W MRI • Focal Nodular Hyperplasia (FNH) • 2nd most common benign hepatic neoplasm (behind hemangioma) • Most commonly occurs in young females (age 20-40) • Questionable/controversial association with use of oral contraceptive pills • Composed of abnormally arranged hepatocytes, bile ducts, and Kupffer cells • Hypervascular, well-circumscribed masses that lack a capsule and contain a central fibrous scar with thick-walled blood vessels • Unlike hepatic adenomas, FNH lesions almost never contain fat or demonstrate hemorrhage, infarction, or necrosis • A single mass is present in approximately 70-80% of cases • Multiple lesions are present in the remaining percentage of cases, with more than four lesions being exceedingly rare • FNH does not have malignant potential and poses little risk other than possible mass effect in large lesions • However, it is important to distinguish this entity from other solid hepatic masses with risk of hemorrhage and malignant degeneration, such as hepatic adenoma, fibrolamellar carcinoma, and hepatocellular carcinoma T1W C+ MRI US CEUS