Download
1 / 51
510 likes | 674 Views
Thoracic and Lumbar Spine Clinical Evaluation. Orthopedic Assessment III – Head, Spine, and Trunk with Lab PET 5609C. Clinical Evaluation. History: Location of Pain: Pain radiating into extremities Peripheral paresthesia or numbness:

E N D
Thoracic and Lumbar Spine Clinical Evaluation Orthopedic Assessment III – Head, Spine, and Trunk with Lab PET 5609C
Clinical Evaluation • History: • Location of Pain: • Pain radiating into extremities • Peripheral paresthesia or numbness: • Result of impingement or pressure on nerve root exiting intervertebral foramen or dural irritation proximal to pain site • Pain Locations: • Lumbar pain – possible ambiguous cause • Sacroiliac pathology – pain around PSIS or radiating pain in hip/groin • Piriformis spasm – symptoms of sciatic nerve dysfunction
History: Onset of Pain: Acute Chronic Insidious pain onset Note: Patient may describe a single incident that initiated pain, although trauma is probably an accumulation or repetitive stresses/microtrauma Clinical Evaluation
History: Mechanism of Injury: Movement: Flexion, Extension, Lateral Bending, Rotation Blunt Trauma: Direct blow to lumbar/thoracic area Contusions Compressive Stress: Hyperextension of spine Clinical Evaluation
History: Pain Consistency: Constant Pain: Unyielding (does not improve with various position of patient’s spine) Example pathology – Inflammation of dural sheath Clinical Evaluation
Clinical Evaluation • History: • Pain Consistency: • Intermittent Pain: • Mechanical Origin – certain spinal positions may ↑ or ↓ pain symptoms • Compression/stretching of nerve root – Increase pain • Positioning (flexion, traction) – lessen the pressure on involved structure
Clinical Evaluation • History: • Bowel or bladder signs: • Does the patient have any bowel or bladder problems? • Incontinence: Loss of bowel or bladder control • May indicate lower nerve root lesions (cauda equina syndrome), or spinal cord injury • Description: urinary incontinence may range from occasionally leaking urine (during cough/sneeze) to having sudden episodes of strong urinary urgency
Clinical Evaluation • History: • Bowel or Bladder Signs: • Cauda Equina Syndrome: • Nerves within the spinal canal have been damaged • Result: nerves supplying the muscles of the legs, bladder, bowel and genitals do not function properly • Patients experience numbness, loss of sensation and pain in the legs, buttocks and pelvic region (damage usually permanent) • Causes: • Spina bifida (abnormality in closure of spinal canal) • Tumors • Injury (spinal fractures) • Intravertebral disc herniation • Vascular (blood vessel) problems or infections of the cauda equina
History: History of spinal injury: Previous injuries: Structural degeneration Predisposition to injury Changes in activity: Exercise habits (intensity levels, duration, frequency) Footwear, running surfaces New bed Clinical Evaluation
General Inspection: Frontal Curvature: Alignment of lumbar, thoracic, cervical vertebrae with patient lying prone or standing Normal alignment – straight Abnormal alignment: Scoliosis – lateral curvature (lumbar and/or thoracic spine) Clinical Evaluation
General Inspection: Scoliosis Signs and symptoms: Uneven shoulders One shoulder blade appears more prominent Uneven waist / 1 hip higher vs. other Leaning to one side Back pain and difficulty breathing (severe scoliosis) Causes: Idiopathic (85% of cases) Underlying neuromuscular disease, leg-length discrepancy, birth defect, fetal development (congenital) Not caused by poor posture, diet, exercise, or the use of backpacks Clinical Evaluation
Diagnosis: Angle: X-ray Normal Spine (0 degrees) Scoliosis: (> 10 degrees) Complications: (severe scoliosis) Lung and heart damage: compression of rib cage against heart, lungs > 70 degrees Back problems Clinical Evaluation
Clinical Evaluation • General Inspection: • Scoliosis Test: Adam’s Forward Bend Test • Patient Position: Standing with hands held in front (arms straight) • Evaluation Procedure: Patient bends forward, sliding hands down the front of each leg • Positive Test: • Asymmetrical hump along lateral aspect of thoracolumbar spine • One shoulder blade appears more prominent • Uneven hips • Implications: • Functional scoliosis: scoliosis present when patient stands straight, disappears during flexion • Structural scoliosis: present during both standing and with flexion
General Inspection: Sagital Curvature: Normal Alignment: Lordotic cervical Kyphotic thoracic Lordotic lumbar Kyphotic sacral Clinical Evaluation
General Inspection: Observation of GAIT: Spinal pain – influence on walking and running gait Slouching Shuffling Shortened gait Clinical Evaluation
General Inspection: Skin Markings: Café-au-lait spots: presence of darkened areas of skin pigmentation Normal (benign) Collagen disease Neurofibromatosis 1 95% of patients will display spots Clinical Evaluation
Clinical Evaluation • General Inspection: • Skin Markings: Sign of Neurofibromatosis-1 • Neurofibromatosis-1: • Autosomal dominant disease • Characterized by formation of neurofibromas (tumors involving nerve tissue) in the skin, subcutaneous tissue, cranial nerves, and spinal root nerves • Implications: growth of tissue along the nerves – puts pressure on affected nerves and cause pain and severe nerve damage • Loss of nerve function (sensation, movement)
Clinical Evaluation • General Inspection: • Breathing patterns: • Irregular breathing (i.e. shallow respirations, pain) • Injury to thoracic vertebrae • Pressure on thoracic nerves • Trauma to ribs, costal cartilage • Bilateral comparison of skin folds: • Asymmetry of natural folds • Causes: muscle imbalance, ↑ or ↓ kyphosis, scoliosis
General Inspection: Kyphosis: Abnormal forward rounding of the upper back (> 40 to 45 degrees) Round back or hunchback Causes: Developmental problems, degenerative diseases (arthritis), osteoporosis with compression fractures, trauma Severe cases: Can affect lungs, nerves, causing pain and other problems Clinical Evaluation
General Inspection: Kyphosis Test: Forward bend test Patient bends forward from the waist while ATC views the spine from the side With kyphosis, the rounding of the upper back may become more obvious in this position Postural kyphosis – the deformity corrects itself when patient lies on their back Clinical Evaluation
Clinical Evaluation • Postural kyphosis: • May improve on its own • Exercises to strengthen back muscles, correct posture, and sleeping on a firm bed • Structural kyphosis: • Caused by spinal abnormalities • Scheuermann's disease: • Developmental disorder that causes a stooped forward or bent-over posture • Affects between 0.5% and 8% of the general population • Osteoporosis-related kyphosis: • Multiple compression fractures • Low bone density
General Inspection: Movement and Posture: Poor posture (standing, sitting, bending) Lordotic Curve: Reduction: Muscle spasm Hamstring tightness Increased: Hip flexor tightness Abdominal weakness Clinical Evaluation
Clinical Evaluation • General Inspection: • Standing Posture: • Lateral shift in trunk and pelvis • Nerve root impingement (lateral shift ↓ pressure) • Erector Spinae Muscle Tone: • Unilateral hypertrophy or atrophy • Faun’s Beard: • Spina bifida occulta
Clinical Evaluation • General Inspection: Spina Bifida • Birth defect that occurs when the tissue surrounding the developing spinal cord doesn't close properly • Spina Bifida Occulta: • Mildest form, results in a small separation in one or more of the vertebrae of the spine (spinal nerves usually not involved – most patients have no signs/symptoms or neurological problems) • Inspection: Faun’s Beard, a collection of fat, a small dimple or a birthmark on the newborn's skin above the spinal defect • Complications: • Minor physical disabilities • Mental strain • Severity: • Size and location of the neural tube defect • Does skin cover the area? • Do the spinal nerves come out of the affected area of the spinal cord?
Clinical Evaluation • Palpation: Thoracic Spine • Spinous Processes • Supraspinous Ligaments: • Fills space between the spinous processes • Costovertebral Junction: • Articulation between ribs and thoracic vertebrae • Only palpable on slender individuals • Trapezius: • Origin to insertion • Rhomboids and levator scapulae lie deep to middle/upper traps • Paravertebral Muscles • Scapular Muscles
1 – Spinous Processes 2 – Supraspinous Ligaments 3 – Costovertebral Junction 4 – Trapezius 5 – Paravertebral Muscles 6 – Scapular Muscles
Clinical Evaluation C7 T1 T2 T3 T4 T5
1 – Spinous Processes 2 – Step-off Deformity 3 – Paravertebral Muscles
Clinical Evaluation • Spondylolisthesis: • Forward slippage of a vertebrae on the one below it • L4 and L5 / L5 and S1 • Affects 5-6% of males, 2-3% of females • Causes: • Strenuous physical activity (weightlifting, gymnastics, football) • Types: • Developmental: • May exist at birth, or may develop during childhood (generally not noticed until later in childhood/adult life) • Acquired: • Degeneration: caused by the daily stresses that are put on spine (i.e. carrying heavy items, physical sports) • Connections between the vertebrae weaken • Single or repeated force
Spondylolisthesis: Grade 1: 25% of vertebral body has slipped forward Grade 2: 50% Grade 3: 75% Grade 4: 100% Grade 5: Vertebral body completely fallen off (i.e.,spondyloptosis) Clinical Evaluation
Symptoms: May be asymptomatic Low back pain (especially after exercise) ↑ lordosis Pain/weakness in one or both legs ↓ ability to control bowel/ bladder functions Tight hamstrings Advanced spondylolisthesis: changes may occur in the way patient stands/walks Clinical Evaluation
Clinical Evaluation • Palpation: Sacrum and Pelvis • Median sacral crests • Iliac crests: • Palpate laterally from PSIS to find iliac crests and anteriorly to locate ASIS (level of symmetry) • Posterior superior iliac spine • Gluteals • Ischial tuberosity • Greater trochanter • Sciatic nerve: • Place thumb on ischial tuberosity and 3rd finger on the PSIS. 2nd finger will fall into sciatic notch (nerve most superficial as it passes by ischial tuberosity) • Pubic symphysis
1 – Median sacral crests 2 – Iliac crests 3 – PSIS 4 – Gluteal muscles 5 – Ischial tuberosity 6 – Greater trochanter 7 – Sciatic nerve 8 – Pubic symphysis
1 – Iliac crest 2 – Tensor fascia latae 3 – Gluteus medius 4 – Iliotibial band 5 – Greater trochanter 6 – Trochanteric bursa
1 – Pubis 2 – ASIS 3 – AIIS 4 – Sartorius 5 – Rectus femoris
Clinical Evaluation • Active Range of Motion: • Flexion and Extension: • Measured with patient standing • Distance from the fingertips to the floor can be measured (accuracy affected by tightness of hamstrings and calf muscles and scapular protraction) • Gravity assists with movement • More accurate than hook-lying position • Abdominal muscles have to overcome weight of the trunk
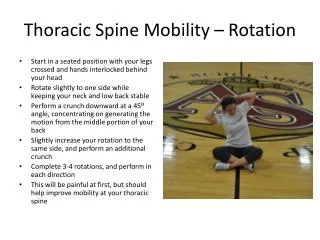
Clinical Evaluation • Active Range of Motion: • Lateral Bending: • Patient standing (feet shoulder width apart and the hand opposite the direction of the movement resting on the ilium) • Patient bends trunk laterally (attempt to tough fingertips to the ground) • Distance between the ground and fingertips is measured • Rotation: • Patient is sitting position (stabilizes pelvis and lower extremity) • Patient rotates shoulder girdles and spinal column (attempt to look behind one’s back) • Movement primarily occurs in thoracic spine
Clinical Evaluation • Passive Range of Motion: • Flexion: • Patient in hook-lying position • Examiner brings the knees to the chest by lifting under the knees and thighs and flexing the hip and thoracic spine • Extension: • Patient prone (hands flat on table at shoulder level – push-up position) • Patient extends arms, lifting the torso (hips and legs remain of table) • Rotation: • Patient in hook-lying position • Patient’s pelvis and legs are rotated to bring lateral portion of the knee towards the table (shoulders remain flat)
Spinal Ligaments Stressed During Passive Range of Motion Testing
Clinical Evaluation • Beevor’s Sign: • Test for thoracic nerve inhibition • Patient performs an abdominal curl-up from hook-lying position • Normal Findings: abdominal muscles receive concurrent innervation from T5-T12 nerve roots (umbilicus does not move) • Positive Test: umbilicus is pulled toward the head • Characteristic of spinal cord injury between T6 and T10 levels • Upper abdominal muscles (rectus abdominis) are intact at the top of the abdomen but weak at the lower portion, patient is asked to do a sit up – only the upper muscles contract (umbilicus pulled toward the head)
Clinical Evaluation • Resistive Range of Motion: • Flexion: • Patient position – supine with knees flexed and feet flat on table • Stabilization – pelvis • Resistance – applied to the superior sternum as patient lifts the scapulae off the table • Muscles tested – rectus abdominis, internal oblique, external oblique
Clinical Evaluation • Resisted Range of Motion: • Extension: • Patient position – prone with arms interlocked behind the head • Stabilization – lower lumbar region • Resistance – applied to upper thoracic spine as patient lifts head, chest, and arms off table • Muscles tested – iliocostalis lumborum, iliocostalis thoracis, longissimus thoracis, spinalis thoracis, semispinalis thoracis, rotators, latissimus dorsi