Download
1 / 31
621 likes | 1.82k Views
Amino Acids Metabolism : Disposal of Nitrogen. No Storage of Amino Acids in the body. So, amino acids must be obtained from Diet De novo synthesis (of non-essential aa ) Degradation of protein (normal turnover). De novo synthesi s. Amino Acids Pool. Diet. Degradation.

E N D
Amino Acids Metabolism: Disposal of Nitrogen
No Storage of Amino Acids in the body • So, amino acids must be obtained from • Diet • Denovo synthesis (of non-essential aa) • Degradation of protein (normal turnover)
De novo synthesis Amino Acids Pool Diet Degradation Protein synthesis Glucose & Fas ..etc Other Nitogen- containing comp.
Protein Turnover Simultaneous synthesis & degradation of protein molecules
Protein turnover Most proteins in the body are constantly being synthesized & then degraded, permitting the removal of abnormal or unneeded proteins
Protein Degradation By Two Major Enzyme Systems 1-Ubiquitin-proteasome mechanism • Energy-dependent • Mainly for endogenous proteins (proteins synthesized within the cell) 2- Lysosomes • Non-energy-dependent • Primarily for extracellular proteins as: - plasma proteins that are taken into cells by endocytosis - cell surface membrane proteins: for receptor-mediated endocytosis
Amino Acids Catabolism - Overview • Unlike glucose and fatty acids, amino acids are notstored by the body • Amino acids in excess of biosynthetic needs are degraded. • Degradation of amino acids involves: First Stage Removal of α-amino group Ammonia(NH3) Second Stage Remaining carbon skeleton Energy metabolism
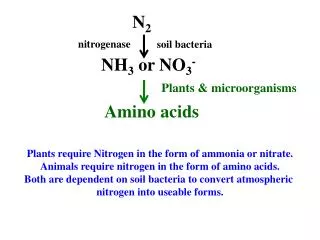
1st phase of catabolism of amino acids: • Removal of the α-amino groups With production of Free Ammonia In Liver Small amount excreted in urine Urea
Amino Acids Catabolism - Overview • Ammoniais produced by all tissues from the catabolism of amino acids • Ammoniais mainly disposed is via formation of urea in liver • Blood level of ammoinamust be kept very low, otherwise, hyperammonemia& CNS toxicity will occur • To solve this problem, ammoniais transported from peripheral tissues to liver via formation of: Glutamine (most tissues) Alanine (muscle)
2nd phase of A. A. catabolism Carbon skeletons of the α-ketoacidsare converted to common intermediates of energy producing, metabolic pathways • ATP, CO2 & H2O (by Citric acid cycle) • Glucose (by gluconeogenesis) • Fatty Acids (from acetyl CoA) • Ketone Bodies (from acetyl CoA)
Amino Acids MetabolismRemoval of Nitrogen from Amino Acids Removing the a-amino group • Essential for producing energy from any amino acid • An obligatory step for the catabolism of all amino acids
Deamination Pathways Amino group (nitrogen) is removed from an amino acid by either 1- Transamination : by transaminases 2- Oxidative Deamination: by glutamate dehydrogenase
1-Transamination ALL Amino Acids (exceptlysine & threonine) • a-ketoglutarateaccepts the • amino group from amino acids to • become glutamate by: • Transaminases (aminotransferases) • Glutamate: • Glutamate dehydrogenase • Ammonia Transaminase Energy, glucose, FAs or KB
2-Oxidative deamination by Glutamate Dehydrogenase Glutamate(from transamination steps) by enzyme Glutamate Dehydrogenase Ammoniaa-ketoglutarate Urea Cycle Urea used for transamination of further amino acids
Diagnostic Value of Plasma Aminotransferases • Aminotransferases are normally intracellularenzymes • Plasma contains low levels of aminotransferases representing release of cellular contents during normal cell turnover • Elevated plasma levels of aminotransferases indicate damage to cells rich in these enzymes (as physical trauma or disease to tissue) • Plasma AST & ALT are of particular diagnostic value
Diagnostic Value of Plasma Aminotransferases 1- liver disease: Plasma ALT & AST are elevated in nearly all liver diseases but, particularly high in conditions that cause cell necrosis as: viral hepatitis toxic injury prolonged circulatory collapse ALTis more specificfor liver disease than AST ASTis more sensitive(as liver contains a large amount of AST) 2- Nonhepatic disease: as: Myocardial infarction Skeletal muscle disorders These disorders can be distinguished clinically from liver disease
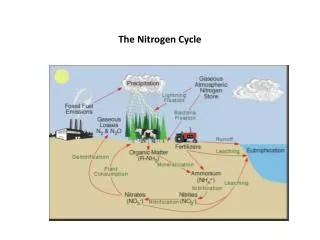
Metabolism of Ammonia Ammonia is produced by all tissues during metabolism of a variety of compounds Ammoniais disposed of primarily by formation of urea in the liver The level of ammonia in bloodmust be kept very low Slightly elevated concentrations (hyperammonemia) are toxic to CNS So, There must be a mechanism by which Ammonia is moved from peripheral tissues to the liver for disposal as urea While at the same time Ammonia must be maintained at low levels in blood
Disposal of Ammonia 1- Urea in the liver • is quantitatively the most important disposal route for ammonia • Urea is formed in the liver from ammonia (urea cycle) • Urea travels in the blood from the liver to the kidneys where it is filtered to appear in urine
Disposal of Ammonia cont. 2- Glutamine in most peripheral tissues especially brain, sk.ms. & liver • In most peripheral tissues, glutamate binds with ammoniaby action of glutamine synthase • in the brain, it is the major mechanism of removal of ammonia from the brain • This structure provides a nontoxic storage & transport form of ammonia • Glutamine is transported to blood to other organs esp. liver & kidneys • In the liver & Kidney, glutamine is converted to ammonia & glutamate by the enzyme glutaminase.
Disposal of Ammonia cont. 3-Alanine in skeletal muscles • Ammonia + Pyruvate form alanine in skeletal muscles • Alanine is transported in blood to liver • In liver, alanine is converted to pyruvate & ammonia • Pyruvate can be converted to glucose (by gluconeogenesis) • Glucosecan enter the blood to be used by skeletal muscles(GLUCOSE - ALANINE PATHWAY)
Disposal of Ammonia cont. Glutamine in Most Tissues Esp. brain & Kidneys Urea in Liver Alanine in Skeletal Muscles
Urea Cycle • Urea is produced in the liver • From the liver, it is transported in the blood to the kidneys for excretion in urine Urea is composed of: Two nitrogen atoms • First nitrogen atom is from free ammonia • Second nitrogen atom is from aspartate Carbon & oxygen atoms are from CO2
Reactions of the Urea Cycle • First two reactions occur in the mitochondria • Remaining reactions occur in the cytosol Ammonia + Aspartate + CO2+ 3 ATP UREA+Fumarate+ 2 ADP + AMP + 2 Pi +PPi+ 3 H20 • Synthesis of urea is irreversible • 4 high-energy phosphates are consumed for synthesis of one molecule of • urea
Fate of Urea Urea (synthesized in the liver) Blood Kidneyintestine Urinecleaved by bacterial urease Ammonia CO2 In stool Reabsorbed in blood
Hyperammonemia= Increase of ammonia level of blood • Blood Ammonia • Normal level of blood ammonia is 5-50 mmol/L • Hyperammonemia A medical emergency as ammonia has a direct neurotoxic effect on CNS • Ammonia intoxication: • It is defined as toxicity of the brain due to increase in ammonia level in the systemic blood. • This increased ammonia will be directed to αketoglutarateto form glutamic acid then glutamine leading to interference with citric acid cycle so decrease ATP production in the brain cells. Clinical manifestations: Tremors, slurring of speech, somnolence, vomiting, cerebral edema & blurring of vision At high concentrations, ammonia can cause coma & death
Types of Hyperammonemia 1- Acquired Hyperammonemia 1-Liver diseases: are common causes in adults 1- Acute causes: viral hepatitis, ischemia, hepatotoxins 2- Chronic causes: liver cirrhosis due to alcoholism, hepatitis, biliary obstruction…etc may result in the formation of collateral circulation around the liver So, portal blood is shunted directly into systemic circulation & detoxication of ammonia to urea is markedly impaired 2- Gatrointestinal Bleeding By action of bacteria of GIT on blood urea with production of big amounts of ammonia that is absorbed to blood.
Types of Hyperammonemia cont. 1-Hereditary Hyperammonemia Genetic deficiencies can occur for each of the five enzymes of the urea cycle (overall prevalence 1:300,000 live births) Ornithine transcarbamoylase deficiency • X-linked • Most common deficiency among all 5 enzymes • Males are predominantly affected • Females carriers are clinically affected All other urea cycle disorders are autosomal recessive • In each case, failure to synthesize urea leads to hyperammonemia during the first weeks following birth • All inherited disorders of the urea cycle enzymes result in mental retardation
Treatment of Hyperammonemia • Limiting protein in diet • Administration of compounds that bind covalently to amino acids To produce nitrogen-containing molecules that are excreted in the urine for example: Phenylbutyrategiven orally converted to phenylacetate that condenses with glutamine to form phenylacetylglutaminewhich is excreted in urine
Hyperammonemia in Renal Failure Rena Failure blood urea levels are elevated Transfer of urea to intestine is increased Much amounts of Ammonia is formed by bacterial urease Absorbed to blood Hyperammonemia • To reduce hyperammonemia: Oral neomycin reduces the amount of intestinal bacteria responsible for ammonia production