Download
1 / 32
320 likes | 653 Views
PURPOSE. Understand functions of skinUnderstand inflammation in skinUnderstand types of dermatitisHow it is diagnosedHow it is treated. FUNCTIONS OF SKIN. Protect against infections, chemical toxins and physical agents (UV, ionizing radiation)Prevent insensible water lossControl body temperature (thermoregulation)Sensation, communication (psychosocial, sexual, endocrine functions)Self-regeneration and healing.

E N D
1. DERMATITIS AND ECZEMA:ITCHING FOR ANSWERS Anthony A. Gaspari, MD
Shapiro Professor and Chair
Department of Dermatology
University of Maryland School of Medicine
3. FUNCTIONS OF SKIN Protect against infections, chemical toxins and physical agents (UV, ionizing radiation)
Prevent insensible water loss
Control body temperature (thermoregulation)
Sensation, communication (psychosocial, sexual, endocrine functions)
Self-regeneration and healing
4. TERMINOLOGY Dermatitis = Dermat + itis
refers to skin means
�inflamed�
(thus, inflamed skin)
Other examples: arthritis, colitis,
encephalitis, etc.
5. TERMINOLOGY
6. CARDINAL FEATURES OF INFLAMMATION Calor (warmth) - increased blood flow
Rubor (redness) -dilated blood vessels
Dolor (pain)- irritation of nerves in inflamed tissues
7. TYPES OF DERMATITIS Allergic contact dermatitis
Irritant contact dermatitis
Atopic dermatitis
Other types
8. IMPACT OF CONTACT DERMATITIS T-lymphocyte-mediated type IV allergic reaction
Commonest specific skin disorder encountered
Second commonest dermatosis encountered in Dermatologist office
30% of all occupational disease
USA annual cost $250 million/year
10. COMMON ALLERGENS Nickel Jewelry, foods
Benzocaine anesthetics
Fragrance perfumes, personal care products
Mercaptomix rubber gloves
Black rubber mix rubber gloves
PPD black hair dye
Potassium dichromate leather, spackling, detergents
Cinammic aldehyde fragrance,toothpaste
Quaternium 15 preservative personal care products
11. TREATMENT OF ACD Avoidance!
Avoidance!
Avoidance!
Other
12. TREATMENT OF ACD Topical glucocorticoids
Oral antihistamines
Compresses
Topical Emollients
Oral antibiotics
Oral glucocorticoids
13. IRRITANT CONTACT DEMATITIS Non-immunologic inflammatory reaction of the skin due to an external agent
Varied morphology
Clinical types
Chemical burns
Irritant reactions
Acute irritant contact dermatitis
Chronic irritant contact dermatitis
14. COMMON IRRITANTS Water
Skin cleansers
Industrial cleaning agents
Acids and alkalis
Oils and organic solvents
Oxidizing and reducing agents
Plants
Animal products
Miscellaneous
15. CLINICAL EFFECTS OF IRRITANTS Dermatitis
Ulcerations
Acneiform rashes
Miliaria
Disorders of pigmentation
Alopecia
Urticaria
Granulomas
16. TREATMENT OF ICD Define/remove exposures
Moisturizers
Barrier creams
Topical glucocorticoids
Oral antihistamines
17. ATOPIC DERMATITIS Common immune-mediated inflammatory skin disorder
Prevalence in general population in Western industrialized countries: 10-20%
Multi-factorial etiology
Interactions of genes and environment
Family history of disease usually positive for affected blood relatives
AD genes localized to certain chromosomes-known genes in these areas control immune response and inflammation
18. EPIDEMIOLOGY OF ALLERGIC DISEASES Tenfold regional differences in the prevalence of asthma and atopic diseases
Allergic diseases more common in westernized environments
Asthma and allergy less common in children of animal farmers
Asthma and atopy less common in younger siblings
Asthma and atopy less common in households with dogs as pets
19. CLINICAL CHARACTERISTICS:AGE AT DIAGNOSIS
20. ATOPIC TRIAD
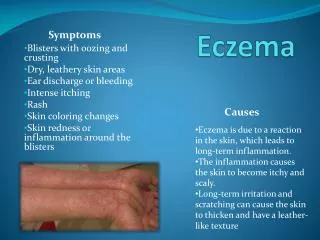
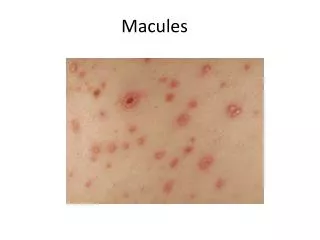
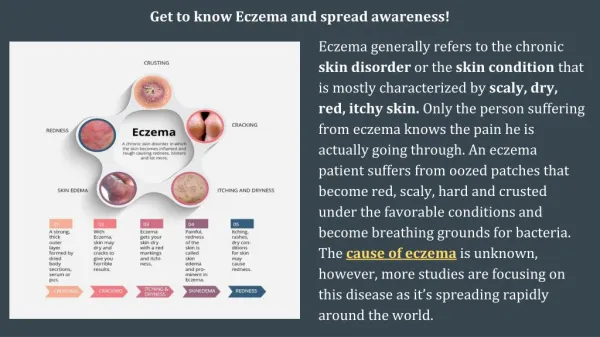
21. ATOPIC DERMATITIS:SIGNS AND SYMPTOMS Pruritus (itching)
Dry, scaly skin
Crusted rashes on face, scalp, hands, arms feet or legs
Small bumps that open and weep when scratched
Redness and swelling of the skin
Thickening of the skin (with chronic dermatitis)
22. ATOPIC DERMATITIS:SIGNS AND SYMPTOMS Location of Dermatitis
Back of knees and bend of elbows
Face
Outer part of ankle
Neck
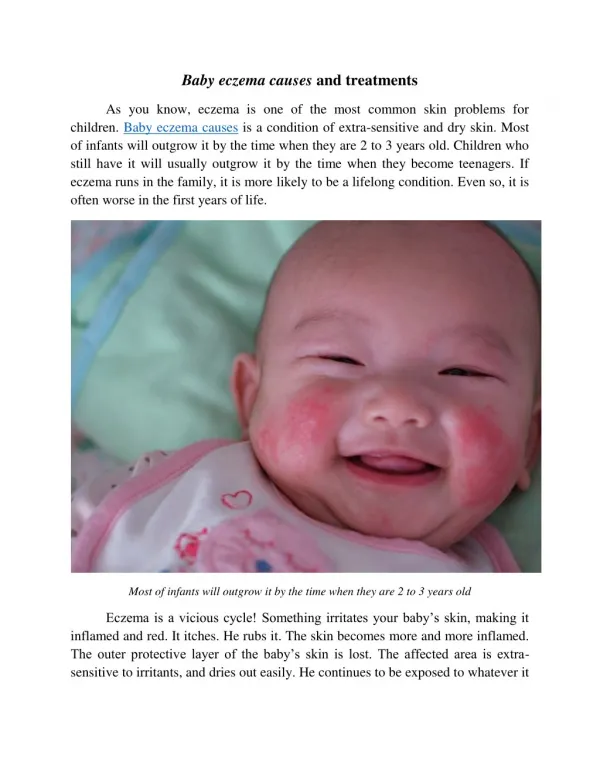
23. CHILDHOOD ECZEMA
25. ATOPIC DERMATITIS:EXACERBATING FACTORS(TRIGGERS) Anxiety/stress
Climatic factors
Temperature
Humidity
Irritants
Detergents/solvents
Wool or other rough material
Perspiration
Allergens (contact, inhalant & food)
Infections (staph and strep)
26. FLARE FACTORS IN ATOPIC DERMATITIS
27. TREATMENT OF ATOPIC DERMATITIS Identify and control �flare factors�
Topical treatments
Glucocorticosteroids
Newer �non-steroidal� TIMs
Emollients
Moisturizers
Baths with added lubricants
Systemic treatments
Oral antihistamine (a cornerstone of treatment)
Oral antibiotics
Systemic steroids
Immunosuppression (phototherapy, cytotoxic drugs)
28. LIMITATIONS TO TOPICAL STEROID THERAPY Efficacy (do they work as they should?)
Skin side effects
Atrophy
Telangiectasia
Striae
Perioral dermatitis
Risk of cataracts and glaucoma
Cushing syndrome and growth retardation
HPA-axis suppression
29. TOPICAL STEROID PHOBIA In patients with AD:
73% worried about corticosteroid usage
24% admit non-compliance due to worry
Key concerns:
Skin thinning (35%)
Non-specific long-term effect (24%)
Absorption/effect on growth (10%)
Br J Dermatol 2000;142:931
30. TOPICAL GLUCOCORTICOIDS
31. TOPICAL IMMUNE MODULATORS Two new agents: Tacrolimus (Protopic) 0.1% ointment Pimecrolimus (Elidel) 1.0% cream
Derived from fungal polypeptides and Inhibit T-lymphocyte activation; Potent immunosuppressive if given systemically
Demonstrated to be effective in childhood and adult AD
Don�t cause atrophy of the skin or other steroid side effects
Slow acting anti-inflammatory
Causes stinging and burn at initiation of therapy; slight increase in skin infections ? Long-term safety not known
32. SUMMARY