Download
1 / 7
70 likes | 242 Views
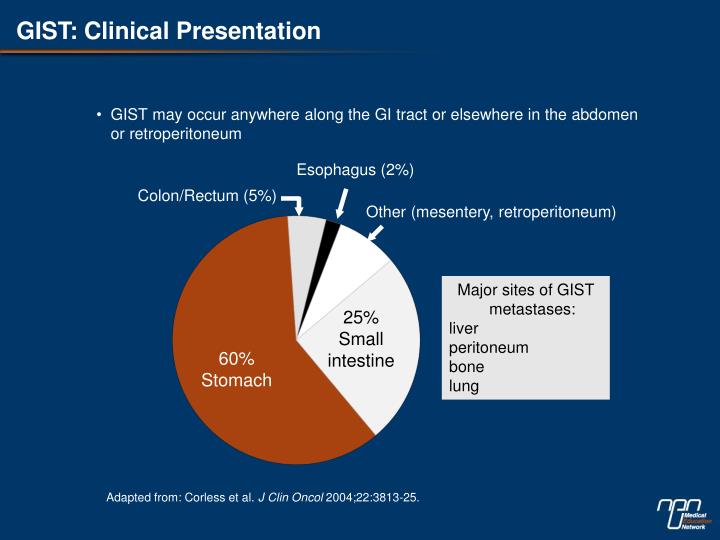
GIST: Clinical Presentation. GIST may occur anywhere along the GI tract or elsewhere in the abdomen or retroperitoneum. Esophagus (2%). Colon/Rectum (5%). Other (mesentery, retroperitoneum). 8%. Major sites of GIST metastases: liver peritoneum bone lung. 25% Small intestine. 60%

E N D
GIST: Clinical Presentation • GIST may occur anywhere along the GI tract or elsewhere in the abdomen or retroperitoneum Esophagus (2%) Colon/Rectum (5%) Other (mesentery, retroperitoneum) 8% Major sites of GIST metastases: liver peritoneum bone lung 25% Small intestine 60% Stomach Adapted from: Corless et al. J Clin Oncol 2004;22:3813-25.
GIST Evaluation Factors for Consideration • GIST histologic type (spindle/epithelioid/mixed) • KIT-positive/-negative • Biologic risk potential (low/intermediate/high) • Tumour size and location (1 section/1 cm tumour) • Cellularity (low/moderate/high), cellular atypia (mild/moderate/marked) • Mitotic count/50 HPF • Tumour necrosis • Mucosal ulceration • Lympho-vascular invasion • Margin status AdaptedfromMarginean C. GIST Consensus Meeting 2007, Ottawa.
RTK Mutation Frequencies KIT (80%) PDGFRA (5-8%) Exon 8 (<1%) Exon 9 (10%) Exon 12 (1%) Exon 11 (67%) Exon 13 (1%) Exon 14 (<1%) Exon 17 (1%) Exon 18 (5%) Adapted from Hurlbut D. GIST Consensus Meeting 2007, Ottawa.
GIST Imaging • CT • Delineates the large exophytic masses and local and distant metastases • Guides tissue biopsy • PET • Differentiates tissues and assesses tumor metabolic activity • For early treatment-response evaluation Large heterogeneous duodenal GIST (D) with multifocal hepatic metastases (M). The biliary tree and pancreatic duct are not dilated. Image reprinted with permission from Lau et al. ClinRadiol 2004;59:487-98.
Primary GIST: Risk Factors for Recurrence After Surgery Tumour size 1.0 Rates of RFS were predicted by mitotic index and tumour size <5 cm 0.75 5-10 cm Mitotic index 0.50 Recurrence-free survival >10 cm 1.0 3 mitoses/30 HPF 0.25 0.75 P=0.03 >3 to 15 mitoses/30 HPF 0 Recurrence-free survival 0.50 0 20 40 60 80 Months 0.25 >15 mitoses/30 HPF P=0.0001 0 0 20 40 60 80 Months Singer et al. J ClinOncol 2002;20:3898-905. Adapted with permission from ASCO.
ACOSOG Z9001 Study: Relapse Events at One Year P=0.0000014 The ACOSOG Z9001 Study, which randomized 644 patients to a TK inhibitor or placebo after GIST surgical resection, was halted early when the relapse rate was 67.5% lower at one year in the arm receiving the TK inhibitor (hazard ratio=0.325;P=0.0000014 for active treatment vs. placebo). Adapted from: DeMatteo et al. ASCO 2007, Abs 10079.
Treatment Algorithm for Patients with Primary Metastatic or Recurrent GIST Primary disease Recurrent disease Metastasisor unresectable No metastasis Imatinib Surgery Progression Response or stable disease Post-operativeimatinib (adjuvant) Under clinical investigation: - Nilotinib- RAD001- PKC412 Sunitinibor surgery? Surgery? Adapted from van derZwan SM, DeMatteo RP. Cancer 2005;104:1781-8.