Download
1 / 33
330 likes | 344 Views
This article discusses the decision-making process at the end of Phase II studies from a regulator's perspective. It explores the factors that influence sponsor's decision making and the need for better risk elucidation and quantification. The article also highlights the decreasing efficiency of drug development and proposes hypotheses for more efficient development programs and data collection. The use of modeling and simulation in decision making is also discussed.

E N D
A regulator’s view of end of Phase II decision making and phase II studies Dr David Wright Senior Statistical Assessor and Scientific Advice Coordinator MHRA
Contents • Sponsor’s decision making at End of Phase II- a view from an interested methodologist • Are the right Phase II studies being done?
Sponsor’s decision making at End of Phase II • Regulators rarely see company decision making strategies • Experience based on hundreds of development programmes (albeit a biased subset; better programmes, better medicines) and scientific advice requests. Also, formal and Informal discussions with senior colleagues in clinical development teams in pharma. • Drug development is risky. The risk is primarily the sponsor’s to bear (as is the profit) • The question is whether risks can be better elucidated, better quantified to aid expert decision making.
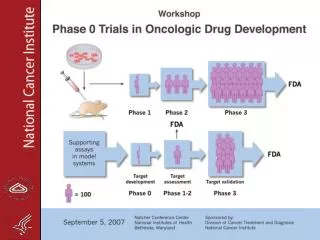
Industry R&D Expense($ Billions) Annual NMEApprovals R&D Investment NME & Biologics Approvals Decreasing efficiency of drug development Source:PhRMA, FDA, Lehman Brothers; [Dr. Robert Ruffolo]
Decreasing efficiency of drug development • Multiple possible causes … • High Phase III failure rate, reasons include: • Inadequate efficacy • doesn’t beat placebo • not competitive in marketplace • Emerging toxicity • Inadequate B-R • Lots of Phase II questions – demonstrate activity, quantify dose-response, what dose, will we beat placebo, what effect size, what toxicity profile, how do efficacy and safety change in broader patient population, …? Ultimately go / no-go decision. • Impossible to address in the same design
Sponsor’s decision making at End of Phase II • Hypothesis 1: Exploratory development programmes are shrinking and are not fit for purpose. Increasing exploratory development (‘learn’) will reduce failure rate in confirmatory trials. • Hypothesis 2: Information needs to be collected efficiently. Novel clinical trial designs add to the ‘toolkit’ and will bring benefits in some indications / development programmes. There is the possibility for adverse effects of novel approaches in other experimental situations. There are many improvements that could be made to the current paradigm without being ‘novel’. • Two questions for Phase II: • With what certainty (how much data) do we wish to address each question of interest? • How can we collect the data efficiently? • Focus of many current discussions seem to be only on hypothesis 2
Sponsor’s decision making at End of Phase II • The tools exist to help quantify the risks being taken to best inform expert (clinical, statistical, regulatory, health-technology etc.) judgement • - Benda N, Branson M, Maurer W, Friede T (2009) Clinical Scenario Evaluation: A framework for the evaluation of competing development strategies. Drug Development 4: 84-88. • Could help to increase likelihood of success, identify early kills and conduct development more efficiently across a portfolio • Could help to move from high risk, high reward to lower risk, high reward?
Sponsor’s decision making at End of Phase II • Also increased use of modelling and simulation • - Help quantify what is known • - Use to guide planning • - Use to replace clinical trial data
Personal reflections on these hypotheses • “Current paradigm unsustainable – must be more efficient” • Efficient OED – “do same for less” • NOT “do less” • Search for ‘efficiency’ concentrates on Phase II and Phase III. Is reducing amount of late Phase II data ‘efficient’ or simply ‘less’? In particular will this reduce Phase III failure rates? • Some arguments in favour of late phase exploratory data being more extensive than in the past … • Increased cost of Phase III trials • More competition (nth statin, mth triptan) • More hurdles (e.g. cost effectiveness, risk-averse / questioning society)
Personal reflections on these hypotheses • Simulation work has shown that ‘optimal’ dose is rarely identified by a standard phase II trial. • Innovative Approaches for Designing and Analyzing Adaptive Dose-Ranging Trials Bjorn Bornkamp et al, Journal of Biopharmaceutical Statistics, Volume 17, Issue 6 November 2007 , pages 965 - 995 • Clinical team metrics include Phase III FPE
Are the right Phase II studies being done? • “The changes in effect of fixed dose studies of recently approved antidepressants employing low and high doses showed that the effect tends to be smaller at higher doses compared with lower doses: • Demonstrating that effect size is not a good predictor of effectiveness of higher antidepressant doses.”
What did they mean? • Probably referring to data like this: • Fixed dose trials • Change from baseline in HAM-D: • Placebo: -10.1 • 10mg: -8.9 • 20mg: -12.4 • 30mg: -11.5 • 40mg: -11.5
SSRI expert working group • Report of the CSM expert working group on the safety of selective serotonin reuptake inhibitor antidepressants • EWG consists of experts and lay members from across the UK • Chair: Professor Ian Weller – University College London • Group included consultant psychiatrists for both child & adolescent and adult patients, professor’s of statistics, epidemiology, psychiatry, patient representatives. • Expert testimony given by patient user groups
SSRI expert working group • Driven by concerns regarding increased “suicidality” in children and adolescents taking SSRIs • Went on to become a wider review of the drug class • Including pharmacovigilance, clinical pharmocology, children and adolescents, suicidal behaviour, withdrawal reactions, dose response – Chapter 9 • Group started May 2003 – report issued December 2004
Dose finding • There was a concern, in the light of the potential AEs that were being investigated, whether the dosing was appropriate • If an AE profile is “clean” maybe there is less concern about precise dosing levels • Usage databases suggested that many patients were being started on higher than the recommended dose • Licence holders were asked to provide the data which supported dosing statements for fresh review by the EWG
Typical SSRI licence • Most SSRI dosing recommendations of the form: • Recommended dose x mg • Patients responding adequately to x mg may increase their dose in increments of y mg to a maximum of z mg • Starting doses established as efficacious • What is the basis for the recommendation to try higher doses if the lower doses fail?
What did we typically see? • Supporting data was usually a mixture of: • Fixed dose studies • Flexible dose studies
Fixed dose studies • Patients randomised to one of a range of doses (or placebo) • Problem: • In many early trials patients were not titrated to higher doses, but started on them straight away • This was corrected in later years • Some companies adjusted by including only patients who lasted for a certain duration on treatment
Fixed dose studies • Often the trend favoured lower doses over higher doses • This doesn’t prove that failing patients will not respond to an increase in dose • But certainly doesn’t prove that they will! • Not studying the situation that we’re interested in • Conclusion: Do allow some comparison between doses – a positive trend would provide some support for up-titration
Flexible dose studies • Patients have their daily dose increased or decreased based upon response • Placebo control (also “increased” and “decreased”) • Mimics the way treatment used in practice
Flexible dose studies • Useful: • Ideal for testing whether a proposed strategy is efficacious • Not so useful: • Cannot tell us whether dose increases are beneficial
Flexible dose studies • Generally patients are titrated to the higher doses in these trials: • But that does not been it was necessary to use them • Do not know what would have happened if dose had NOT been increased
Flexible dose studies • Patients generally improve with time (even on placebo) • Effect of dose increases confounded with time • Also dose increase is “open” – patients know they have increased and this may influence response – attempt to analyse before and after change • Although there is a control arm there is no control for the dose increases
Flexible dose studies • Useful for marketing – tell us whether higher doses would be used if available! • Conclusion: Provide no information to support dose increases
Randomised non-responder trials • All patients start on “low” dose • Patients not responding randomly assigned to increase dose or stay on current dose • Dose increase blinded and controlled
Randomised non-responder trials • Rarely seen • Ideal design to assess the problem • Experience • One drug: No difference (trend favoured no change) • Another (in paediatric trial): large positive trend
Results • “For the majority of SSRIs in the treatment of depressive illness, clinical trial data do not show an additional benefit from increasing the dose of an SSRI above the recommended daily dose” • Expert working group report summarised where they felt recommendations were justified and where they weren’t • Text added to relevant SmPCs stating that benefits of up-titration not demonstrated in clinical trials
Evidence of what happens • Usage data – patients started on higher doses • Quick titrations • Personal experience – prescribers very keen on quick up-titration (even in presence of adverse events) • Evidence base not good that this is correct strategy
Why? • Prescribers personal experiences • “Treating the physicians” – sometimes referred to in cancer as well • Problem – important adverse events difficult to distinguish from lack of efficacy e.g. suicidality, agitation • This makes up-titration dangerous in some cases • Will EWG report influence things over time?
Differences between treatments • Some treatments showed positive trend – others did not • Implausible? • Could be at different part of dose response curve • Products are difference (or they would all have same name) • Don’t definitively understand the mechanisms of how depression occurs – or why SSRIs work
Conclusion • Null-hypothesis disproves the data! • Very informative prior! • Some up-titration decisions based upon an assumption that this is correct • But maybe titration is appropriate – with the data we have we cannot know for certain • But it would be nice to see some randomised non-responder trials to find out!
Conclusion • Voltaire (in 1759) advocated the induction of ideas from concrete • evidence • Pangloss wilfully ignores any evidence that contradicts his initial opinion • Dosing of SSRIs may be a little Panglossian corner of the evidence based medicine world
Conclusions • End of Phase II decision making and design of Phase II studies: • Increasing scope of exploratory development programmes should decrease phase III failure rate. Potential ‘pay-off’ for requirements in phase III. • There is a role for increased use of quantification in company decision making • Choose design of Phase II studies carefully.