Download
1 / 23
230 likes | 252 Views
Learn how to improve performance projects using the PDSA Cycle. Dive deep into identifying, prioritizing barriers, and planning interventions effectively. Discover key strategies and tools for successful implementation and evaluation. 8

E N D
Plan−Do−Study−Act!Using the PDSA Cycle to Improve Your Performance Improvement Projects March 18, 2014 Presenter: Christi Melendez, RN, CPHQAssociate Director, Performance Improvement ProjectsHealth Services Advisory Group, Inc.
Performance Improvement Principle • Your current systems and improvement strategies have resulted in your current outcomes. • What you’re doing is getting you the results you have. • To GET different results, you have to DO something different.
Selecting Changes While all changes do not lead to improvement, all improvement requires change. What changes can you make that will result in improvement?
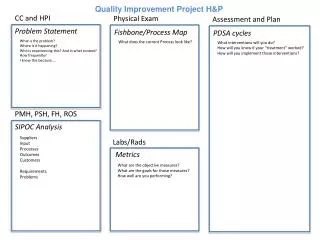
Identifying Barriers • Conduct an initial barrier analysis to identify possible barriers. • Brainstorming and the “Five Whys” • Fishbone Diagram • Key Driver Diagram
Prioritizing Barriers • Request data related to identified barriers. • Evaluate whether data support barriers’ relevance. • Rank barriers—from highest to lowest priority.
Plan Interventions Development of Interventions Avoid “Passive” Interventions • Mailers • Reminder letters • Newsletter articles • Postcards, flyers, and brochures • Updating Web site/portals • Robot calls
Plan Interventions (cont.) Develop “Active” intervention(s) that directly address prioritized barriers and will impact indicator outcomes. • Face-to-face education efforts (enrollee and provider) • Outreach events—“boots on the ground” • Policy/process changes • Performance report cards • Incentive programs (enrollee and provider)
PDSA Cycle • Develop a strategy to implement the interventions. • Develop a plan to test the intervention (Who? What? When? Where? What data need to be collected?)
PDSA Cycle (cont.) • Try the intervention on a small scale. • Carry out the intervention as designed. It’s better to do a few interventions well!
PDSA Cycle (cont.) • Evaluate the effectiveness of the intervention. • Analyze your results. • What did you learn? • What were the results compared to your prediction?
PDSA Cycle (cont.) • Use what you learned from the evaluation/analysis. • Refine or revise. • Determine next steps. • If successful, how will the intervention be rolled out on a larger scale? • If unsuccessful, repeat the cycle.
What It Takes to Get Improvement Improvement will not happen without these components: • Will • Ideas • Execution
Setting Goals What are you trying to accomplish? The goal should be “S-M-A-R-T”. Specific Measurable Attainable Relevant Time-bound
Managed Medical Assistance (MMA) Statewide PIPs There are two statewide PIPs: • Preventive Dental Services for Children • Improving Prenatal Care and Well-Child Visits in the First Fifteen Months of Life—Six or More Visits
Preventive Dental Indicator PIP Title: The percentage of enrollees 1 to 20 years of age who had at least one preventive dental service during the measurement year. Numerator: Total number of unduplicated enrollees 1 to 20 years of age who had at least one preventive dental service under the supervision of a dentist. Codes: D1000—D1999. Denominator: Eligible enrollees 1 to 20 years of age who have been continuously enrolled in Medicaid or Children’s Health Insurance Program (CHIP) Medicaid Expansion programs for at least 90 days and are eligible to receive Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) services.
Prenatal/WCV PIP Four Potential Study Indicators Potential Study Indicator #1 Title: The percentage of women who had a live birth and received a prenatal care visit as an enrollee of the MMA plan in the first trimester or within 42 days of enrollment in the health plan. Numerator: Total number of women who had a live birth and received a prenatal visit in the first trimester or within 42 days of enrollment. Denominator: Eligible women who delivered a live birth on or between November 6 of the year prior to the measurement year and November 5 of the measurement year.
Prenatal/WCV PIP (cont.) Potential Study Indicator #2 Title: The percentage of women who had a live birth and received greater than or equal to 81 percent of expected prenatal visits. Numerator: Total number of women who had an unduplicated count of greater than or equal to 81 percent of the number of expected prenatal visits (adjusted for the month of pregnancy at time of enrollment and gestational age). Denominator: Eligible women who delivered a live birth on or between November 6 of the year prior to the measurement year and November 5 of the measurement year.
Prenatal/WCV PIP (cont.) Potential Study Indicator #3 Title: The percentage of women who received a full course of antenatal steroids completed prior to delivering a live, preterm newborn(s). Numerator: Total number of women who received a full course of antenatal steroids completed prior to delivering a live, preterm newborn(s). Course of steroids must be completed prior to date of delivery. Denominator: Women enrolled in the MMA plan delivering a live, preterm newborn(s) with >=24 and <32 weeks gestation completed.
Prenatal/WCV PIP (cont.) Potential Study Indicator #4 Title: The percentage of children 0−15 months of age who received six or more well-child visits with a Primary Care Physician (PCP) during the measurement year. Numerator: Total number of children who received six or more well-child visits with a PCP during their first 15 months of life. Denominator: Eligible children 0−15 months of age during the measurement year.
Measurement Periods Baseline: January 1, 2014, through December 31, 2014 R1: January 1, 2015, through December 31, 2015 R2: January 1, 2016, through December 31, 2016 The eligible population size will be smaller for baseline than subsequent years due to the transition.