Download
1 / 18
180 likes | 327 Views
Objective. At the end of this session the participant will: Recognise some instruments that can be used to measure the outcomes of co-morbidity management Value an approach to teaching and learning about measuring outcomes of co-morbidity management. Introduction.

E N D
Objective At the end of this session the participant will: • Recognisesome instruments that can be used to measure the outcomes of co-morbidity management • Value an approach to teaching and learning about measuring outcomes of co-morbidity management
Introduction • Outcome measures traditionally have been disease-specific • It is the difficult to measure health status and clinical outcomes at the level of the whole person • The common presence of multiple co-morbidities renders single-disease outcomes inadequate for evaluating the quality of a generalist oriented model of care
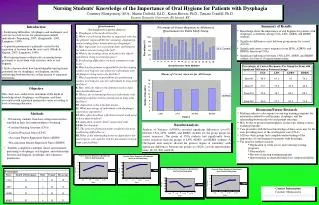
Measuring outcomes of co-morbidity management Jaime Correia de Sousa, MD, MPH Horizonte Family Health Unit Matosinhos Health Centre - Portugal Health Sciences School (ECS) University of Minho, Braga - Portugal
What are our aims in the management of co-morbid patients? • Provide the best available care considering patient’s choices • Adequate management of the health systems’ resources realistic aims with the available logistics • Prevention of health inequities to reduce the economic burden of illness in the individual and in the family
1. Provide the best available care Outcome measures • Impact in physical function • Psychological impact • Measuring quality of life
Impact in physical function • Methods of measuring the outcomes of care have been developed for many chronic diseases • These methods are usually disease specific • Measuring performance indicators health outcomes
Impact in physical function Traditional measures • Mortality • Morbidity • Disability • Length of hospital stay • Hospital readmissions • Remissions • Polymedication We need more specific, patient-centred measures
Impact in physical function WONCA-COOOP Necessary measures • Number of severe and chronic diseases • Measuring disease severity • Measuring the interaction of diseases co-morbid indices • Disease burden sum/ influence of severity of co-morbid conditions
Psychological impact Measurement scales and questionnaires for: • Anxiety • Depression • Substance abuse • Suicide • Psychological impact of chronic diseases
Measuring quality of life Quality of Life (QoL) scales and questionnaires • Short-Form-36 Health Survey (SF 36), SF-20 or SF 12 • Nottingham Health Profile (NHP) • European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) • Duke Severity of Illness (DUSOI) • Quality of Well-Being Scale (QWB)
2. Adequate management of the health systems’ resources Outcome measures • Referral • The use of medication • Access to primary care • The economic burden of co-morbidity in the community
Measuring referral The reasons for the variation in referral rates is poorly understood Referral rates do not correlate well with appropriateness of referral • Number • Characteristics • Appropriateness of referrals • Causes of variation (patient, provider, health care system, social factors, etc) National Primary and Care Trust Development Programme www.natpact.nhs.uk
Measuring the use of medication Some possible areas to measure: • Prescribing profile • Compliance • Accordance to guidelines • Assessment of drug interactions and side-effects (software) • Costs with medicines • Interaction / shared information with pharmacists • Prescription rates for “critical” drugs – antibiotics, tranquillisers, sedatives, analgesics, narcotic analgesics
Measuring access to primary care • Physician’s demographics • Geographic distribution of HC or surgeries • Means of transportation • Appointment systems • Out-of-ours schemes • PHC team • Patient’s questionnaires
The economic burden of co-morbidity • Impact of disease in the community • Health care costs • Sick-leave • Loss of tax revenue Not all dimensions of economic burden can be measured easily
3. Prevention of health inequities Outcome measures • The economic burden of co-morbidity in the individual and the family
The economic burden of co-morbidity • Health inequities • identify unmet needs • unjustified limits to accessibility (socio-economic status, disadvantageous position caused by illnesses) • the Inverse Care Law (Tudor-Hart) • Impact of disease in the individual and the family • direct costs of the disease and treatments • loss of family income
Conclusion • It is the difficult to measure health status and clinical outcomes at the level of the whole person • We need more specific, patient-centred measures instead of the traditional disease specific methods • Some developments have occurred in this area • More research is needed to validate tools and methodologies