Download
1 / 44
830 likes | 3.03k Views
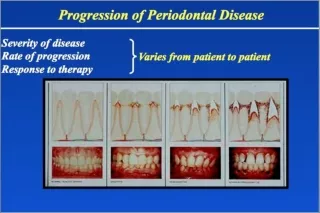
Periodontal risk assessment. Nomenclature Patient associated risk factors Local risk factors. Rio 2003-11. Risk markers : Indicates an increased risk but does not cause the disease- -e.g., age and socio-economic factors Risk factors : Factor that participates in the

E N D
Periodontal risk assessment Nomenclature Patient associated risk factors Local risk factors Rio 2003-11
Risk markers: Indicates an increased risk but does not cause the disease- -e.g., age and socio-economic factors Risk factors: Factor that participates in the initiation and/or progression of the disease, such as smoking and diabetes Rio 2003-11
A risk factor should be modifiable Non-modifiable risk factors are sometimes referred to as Determinants
Patient associated risk factors Genetics Smoking Diabetes Downs syndrome Osteoporosis Other serious diseases Stress Socio-economic conditions Allergies Diet Medication Hyperlipidemia Rio 2003-11
Patient associated risk factors Genetic Twin and family studies show that aprox. 50% of the clinical variation is genetic Polymorfisms (TNFa, IL-1b) HLA Rio 2003-11
Associtaion between genotype and severe peridontitis in non-smokers The risk to have periodontitis was 2 times higher for genotype positive Lätt n=18 Moderat n=37 n=44 Grav % 0 20 40 60 80 Procent genotype positive Kornman et al. 1997
Cytokines and prostaglandins Host response Other virulens factors Pathogenesis of periodontitis Neutrophils Antibodies Clinical changes MMP Complement Tissue degradation Bacterial load Turn over Antigen LPS Serine proteases Oxygen radicals Interleukin +
IL-1 genotype and adult periodontitis • among young New Zealanders • W. M. Thomson, S. J. Edwards, D. P. Dobson-Le, • G. R. Tompkins, R. Poulton, D. A. Knight and A. W. Braithwaite • The aim of this study was to investigate theassociation between adult periodontitis and • IL-1 genotype in apopulation-based sample of 26-year-olds. • 3 disease groups: "Severe"(1+ teeth with 5+mm PD; N = 25), • "Moderate" (2+ teeth with 4+mm PD; N =36), • "Controls" (the remainder; N = 800). • Those with IL-1B(+3953) [1,1]/IL-1A(+4845) [2,2] had • 12.3times the odds of being in the "Severe" group.
Patient associated risk factors Smoking the most important environmental risk factor 2,8 higher risk to get periodontitis Papapanou 1996 14 higher risk to get the disease before 33 years of age Linden et al. 1994, Schenkein et al. 1995 Rio 2003-11
Patient associatedrisk factors Smoking Periodontitis in smokers respond less to treatment Former smokers get a slower disease progression Bolin et al. 1993 Rio 2003-11
Cytokines and prostaglandins Host response Other virulens factors Pathogenesis of periodontitis Neutrophils Antibodies Clinical changes MMP Complement Tissue degradation Bacterial load Turn over Antigen LPS Serine proteases Oxygen radicals Smoking Smoking +
Patient associatedrisk factors Diabetes mellitus Periodontitis is twice as usual No difference between type I and II Periodontitis is considered a complication to diabetes More frequent in patients with other complications Rio 2003-11
Cytokines and prostaglandins Host response Other virulens factors Pathogenesis of periodontitis Neutrophils Antibodies Clinical changes MMP Complement Tissue degradation Bacterial load Turn over Antigen LPS Serine proteases Oxygen radicals Diabetes Diabetes +
Patient associatedrisk factors Downs syndrome Earlier studies show a very high frequency of periodontitis (close to 100%) More recent studies show less but still high One study from Hudding (Modeer et al. 1990) showed that 39% of their patients with Ds (10-19 yrs. old) had periodontitis Rio 2003-11
Patient associatedrisk factors Osteoporosis Good correlation with number of teeth but not with attachment level Rio 2003-11
Patient associatedrisk factors Osteoporosis Common risk factors Rio 2003-11
Stress Several studies indicate an association with an increased risk No conclusive studies Difficult to quantify and to separate from other risk factors Rio 2003-11
Patient associatedrisk factors Allergies - no connection shown Diet-no correlation with minor differences Starvation or severe malnutrition affects the entire body, including the periodontium Medication - hyperplasia No correlation with attachment loss Rio 2003-11
Diet Intake of calcium and Vitamin C have shown a weak correlation with periodontal disease (NHANES).
Patient associatedrisk factors Serious diseases Leukemia Agranulocytosis Neutropenia LAD HIV/AIDS Other very rare genetic disorders Rio 2003-11
Patient associatedrisk factors Hyperlipidemia Significant relationship between hyperlipidemia and periodontitis Lipids increases the reactivity of leukocytes Induced periodontitis increase cholesterol in monkeys Rio 2003-11
?????? Increased leukocyte reactivity Periodontitis Increased plasma levels of IL-1b and TNFa Hyperlipidemia Rio 2003-11
Risk factors Definitive risk factors Genetic Smoking Diabetes Downs syndrome Probable risk factors/markers Stress Osteoporosis Hyperlipidemia Socio-economic conditions Rio 2003-11
Age Rio 2003-11
Is high age a risk factor for periodontitis?
Number of teeth Percentage of dentures 30 40 35 25 30 Age 20 25 20-29 50-59 15 20 75-84 15 10 10 5 5 0 0 300 subjects in each age group Buhlin et al. 2003
Risk of severe periodontal disease in a Swedish adult population. A longitudinal study. Norderyd O. Hugoson A. Grusovin G. Journal of Clinical Periodontology. 26(9):608-15, 1999 Sep 361 individuals in 6 age groups followed for 17 years
Risk of severe periodontal disease in a Swedish adult population. A longitudinal study. Number of teeth 30 25 20 20-30 years 30-40 years 15 40-50 years 50-60 years 60-70 years 10 5 0 1973 1990 Norderyd 1999
Risk of severe periodontal disease in a Swedish adult population. A longitudinal study. Number of teeth lost between 1973 and 1990 3 2,5 20-30 years 2 30-40 years 40-50 years 1,5 50-60 years 60-70 years 1 0,5 0 Norderyd 1999
Risk of severe periodontal disease in a Swedish adult population. A longitudinal study. Bone height % 70 60 50 20-30 years 30-40 years 40 40-50 years 50-60 years 30 60-70 years 20 10 0 1973 1990
Risk of severe periodontal disease in a Swedish adult population. A longitudinal study. Bone loss (%) between 1973 and 1990 6 5 20-30 years 30-40 years 4 40-50 years 50-60 years 3 60-70 years 2 1 0 Norderyd 1999
An epidemiological investigation into the relative importance of age and oral hygiene status as determinants of periodontitis. Abdellatif & Burt 1987 Crossectional study of 14690 north Americans aged 15-74 years (Nahanes I)
An epidemiological investigation into the relative importance of age and oral hygiene status as determinants of periodontitis. Abdellatif & Burt 1987 Conclusion It was concluded that the effect of age on the progression of periodontitis could therefore be considered negligible when good oral hygiene is maintained.
Mean clinical attachment loss by age in six different population samples. Ronderos et al. 2001
Local risk factors Gingivitis Plaque Pocket depth Micro flora Rio 2003-11
Local risk factors Gingivitis Bleeding on probing is not a good marker for disease progression Absence of gingival inflammation is a sign of periodontal health- especially repeated absence Rio 2003-11
Local risk factors Plaque Weak correlation between dental plaque and continuos progression Rio 2003-11
Local risk factors Pocket depth 8 7 6 5 Attachment loss Relative risk 4 Pocket depth 3 2 1 0 0-3 mm 4-5 mm 6-7 mm 8 Rio 2003-11
Local risk factors Micro flora Absence of periopathogens, mainly P. gingivalis (Bacterioides forythus) and A. actinomycetemcomitans, is a sign of periodontal health. Presence, however, is not a predictor for continuos disease progression. Rio 2003-11
Lamina Dura Does the presence or absence of a radiographic crestal lamina dura reflect the clinical status of the periodontium? Rio 2003-11
Assiciation between crestal lamina dura and periodontal status All approximal sites 90 individuals 90 80 70 % 60 Presence 50 Absence 40 30 20 10 CAL BOP PPD visual inflammation Greenstein et al. 1981
The most important risk factor for future disease progression is previous disease Rio 2003-11
Risk profile according Bern Bleeding on probing, % 25 Pocket depth number of pockets 5mm Smoking cig/day 10 19 8 4 ns 4 S 8 0,5 Tooth loss number of lost teeth Systemic disease Diabetes, HIV, leukemia 1,0 Bone height, %/age Rio 2003-11
In conclusion Most important risk factors Genetic Smoking Diabetes Downs syndrome Risk factors associated with disease progression: Bone loss in relation to age Pockets - especially persisting after treatment Gingivitis Plaque Rio 2003-11