Download
1 / 50
500 likes | 647 Views
PCI in diabetics and diffuse disease: role of IIb/IIIa inhibitors. Giuseppe Biondi Zoccai Interventional Cardiology, University of Turin, Italy gbiondizoccai@gmail.com. Disclosure. Co-principal investigator in an upcoming trial on eptifibatide (GSK)

E N D
PCI in diabetics and diffuse disease: role of IIb/IIIa inhibitors Giuseppe Biondi Zoccai Interventional Cardiology, University of Turin, Italy gbiondizoccai@gmail.com
Disclosure • Co-principal investigator in an upcoming trial on eptifibatide (GSK) • No other conflicts of interest or funding to declare
Scope of the problem in DM and diffuse CAD Risk of side branch compromise Overlapping DES Resistance to antiplatelet agents Risk of dissection Prothrombotic milieau Diffuse disease Incomplete revascularization Success (?)
Etiology of peri-procedural necrosis Herrmann, EHJ 2005
Predictors of peri-procedural necrosis Herrmann, EHJ 2005
Modulating factors Herrmann, EHJ 2005
Does peri-procedural necrosis matter at all? Cavallini, EHJ 2005
What is the role of IIb/IIIa inhibitors in PCI of diabetics? • What is the pathophysiology underlying the increased peri-PCI risk of diabetics? • What is the evidence base on of IIb/IIIa inhibitors in diabetics undergoing PCI? • Which additional treatments should be recommended in diabetics or diffuse CAD?
What is the role of IIb/IIIa inhibitors in PCI of diabetics? • What is the pathophysiology underlying the increased peri-PCI risk of diabetics? • What is the evidence base on of IIb/IIIa inhibitors in diabetics undergoing PCI? • Which additional treatments should be recommended in diabetics or diffuse CAD?
Multiple detrimental mechanisms Biondi-Zoccai, JACC 2003
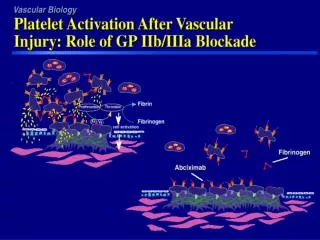
Platelet activation Myers, BUMC Proceedings 2005
Aspirin resistance Hankey, Lancet 2006
Clopidogrel resistance Nguyen, JACC 2005
C vs. T REWARD (Diabetic Sub-study) In-Hospital MACE
What is the role of IIb/IIIa inhibitors in PCI of diabetics? • What is the pathophysiology underlying the increased peri-PCI risk of diabetics? • What is the evidence base on of IIb/IIIa inhibitors in diabetics undergoing PCI? • Which additional treatments should be recommended in diabetics or diffuse CAD?
Reduction in mortality @ 1 month Karvouni, JACC 2003
Survival benefit in DM & ACS Roffi, Circ 2001
ADVANCE trial Valgimigli, JACC 2004
ISAR-SWEET trial DES deployed in only 10% of pts Mehilli, Circ 2004
ISAR-SWEET BARE 31.9% Abc 40.2% Pla P=0.04 DES 7.3% Abc 4.9% Pla P=NS Mehilli, Circ 2004
Paradoxical results of TAXUS IV Teirstein, Am J Cardiol 2005
ISAR-REACT 2 trial DES deployed in 50% of pts Kastrati, JAMA 2006
Prevention of intraprocedural drug-eluting stent thrombosis The occurrence of intra-procedural stent thrombosis (IPST) was analyzed across 1,320 patients undergoing drug-eluting stenting in 4 Italian centers. IPST occurred in 6 (0.5%), with in-hospital major adverse events in 4 (67%). By pooling results of the present study with those of a previous study, for a total of 2,235 patients, elective glycoprotein IIb/IIIa inhibitors appeared to significantly prevent the occurrence of IPST, because no IPST occurred among patients treated with glycoprotein IIb/IIIa inhibitors (0 of 725), whereas all IPST occurred in the absence of adequate upfront IIb/IIIa inhibition treatment (11 of 1,510 [0.7%], odds ratio=0.24 [95% confidence interval 0.06 to 0.97], p=0.036). Biondi-Zoccai, AJC 2005
Prevention of intraprocedural drug-eluting stent thrombosis % Odds ratio=0.24 p=0.034 Biondi-Zoccai, AJC 2005
What is the role of IIb/IIIa inhibitors in PCI of diabetics? • What is the pathophysiology underlying the increased peri-PCI risk of diabetics? • What is the evidence base on of IIb/IIIa inhibitors in diabetics undergoing PCI? • Which additional treatments should be recommended in diabetics or diffuse CAD?
What is the role of IIb/IIIa inhibitors in PCI of diffuse disease? • What is the pathophysiology underlying the increased peri-PCI risk in diffuse disease? • What is the evidence base on of IIb/IIIa inhibitors in patients with diffuse disease? • Which additional treatments should be recommended in diabetics or diffuse CAD?
What is the role of IIb/IIIa inhibitors in PCI of diffuse disease? • What is the pathophysiology underlying the increased peri-PCI risk in diffuse disease? • What is the evidence base on of IIb/IIIa inhibitors in patients with diffuse disease? • Which additional treatments should be recommended in diabetics or diffuse CAD?
Impact of plaque burden Porto, Circ 2006
Predictors of intraprocedural stent thrombosis in the RECIPE Study IPST No IPST Variable n=6 n=1314 P Multiple stenting in the same lesion 3 (50%) 155 (12%) 0.027 Total stent length per vessel 50±42 27±21 0.047 Baseline minimum lumen diameter 0.35±0.350.79±0.46 0.021 Biondi-Zoccai, AJC 2005
Hazards of multivessel DES implantation But: CK-MB 3xULN in 26 (16.8%) patients; specifically 17 [12.8%] with 2VD SES implantation and in 9 [32.1%] patients with 3VD SES implantation Orlic, JACC 2004
47.3 32.9 25.1 25.0 TAXUS V- the impact on side branches in the overlap region (per side branch) Control TAXUS • Possible Causes for TIMI Flow Reduction? • Plaque burden & “snowplow” effect • Jailing of the side branch • Impact of increased strut width Any TIMI Flow Reduction p=0.10 p=0.025 • Macro Strut Width • TAXUS 120 µm • Express2 90 µm • 33% increase in total strut width 51/203 68/207 12/48 26/55 Non-overlap region Overlap region
Hazards of overlapping DES implantation in diffuse disease Tsagalou, JACC 2005
What is the role of IIb/IIIa inhibitors in PCI of diffuse disease? • What is the pathophysiology underlying the increased peri-PCI risk in diffuse disease? • What is the evidence base on of IIb/IIIa inhibitors in patients with diffuse disease? • Which additional treatments should be recommended in diabetics or diffuse CAD?
Mortality at 30 days Karvouni, JACC 2003
Role of IIb/IIIa inhibitors in ACS Consisting of peri-procedural IIb/IIIa inhibitors (p=0.041) and/or thienopyridines (p=0.091) Biondi-Zoccai, Am Heart J 2005
Prevention of acute drug-eluting stent thrombosis % Odds ratio=0.24 P=0.034 Biondi-Zoccai, AJC 2005
What is the role of IIb/IIIa inhibitors in PCI of diffuse disease? • What is the pathophysiology underlying the increased peri-PCI risk in diffuse disease? • What is the evidence base on of IIb/IIIa inhibitors in patients with diffuse disease? • Which additional treatments should be recommended in diabetics or diffuse CAD?
Additional treatments +/- + +++ +++ + +/- +/- Herrmann, EHJ 2005
Superiority of a high (>600 mg) clopidogrel loading dose Outcome: One-month death or myocardial infarction Study High loading Low loading Peto OR Peto OR or sub-category n/N n/N 95% CI 95% CI 01 Randomized trials ALBION 2/68 1/35 1.03 [0.09, 11.50] ARMYDA-2 5/126 15/126 0.34 [0.14, 0.84] CLEAR PLATELETS 1/60 3/60 0.36 [0.05, 2.61] Cuisset 6/146 13/146 0.46 [0.18, 1.15] Subtotal (95% CI) 400 367 0.41 [0.23, 0.75] Total events: 14 (High loading), 32 (Low loading) Test for heterogeneity: Chi² = 0.79, df = 3 (P = 0.85), I² = 0% Test for overall effect: Z = 2.90 (P = 0.004) 02 Non-randomized studies Wolfram 13/319 4/126 1.28 [0.44, 3.74] Subtotal (95% CI) 319 126 1.28 [0.44, 3.74] Total events: 13 (High loading), 4 (Low loading) Test for heterogeneity: not applicable Test for overall effect: Z = 0.45 (P = 0.66) Total (95% CI) 719 493 0.54 [0.32, 0.91] Total events: 27 (High loading), 36 (Low loading) Test for heterogeneity: Chi² = 4.03, df = 4 (P = 0.40), I² = 0.8% Test for overall effect: Z = 2.31 (P = 0.02) 0.01 0.1 1 10 100 Favours high loading Favours low loading Biondi-Zoccai, submitted
What about bivalirudin? Outcome: Death/MI/recurrent ischemia Study DTI Control Peto OR Peto OR or sub-category n/N n/N 95% CI 95% CI 01 Bivalirudin vs heparin plus provisional or routine GPIIbIIIa inhibitors ACUITY 356/4604 334/4603 1.07 [0.92, 1.25] CACHET 4/174 6/94 0.32 [0.09, 1.21] PROTECT-TIMI 30 51/284 82/574 1.32 [0.89, 1.96] REPLACE-1 26/532 30/524 0.85 [0.49, 1.45] REPLACE-2 227/2986 211/3000 1.09 [0.90, 1.32] Subtotal (95% CI) 8580 8795 1.07 [0.96, 1.20] Total events: 664 (DTI), 663 (Control) Test for heterogeneity: Chi² = 5.04, df = 4 (P = 0.28), I² = 20.7% Test for overall effect: Z = 1.25 (P = 0.21) 0.5 0.7 1 1.5 2 Favours DTI Favours control Outcome: Death/MI/recurrent ischemia/major bleeding Study DTI Control Peto OR Peto OR or sub-category n/N n/N 95% CI 95% CI 01 Bivalirudin vs heparin plus provisional or routine GPIIbIIIa inhibitors ACUITY 541/4604 538/4603 1.01 [0.89, 1.14] PROTECT-TIMI 30 52/284 86/574 1.28 [0.87, 1.88] REPLACE-1 38/532 46/524 0.80 [0.51, 1.25] REPLACE-2 275/2975 299/2990 0.92 [0.77, 1.09] Subtotal (95% CI) 8395 8691 0.98 [0.89, 1.08] Total events: 906 (DTI), 969 (Control) Test for heterogeneity: Chi² = 3.36, df = 3 (P = 0.34), I² = 10.7% Test for overall effect: Z = 0.39 (P = 0.70) 0.5 0.7 1 1.5 2 Favours DTI Favours control Abbate, submitted
Eligibility : DM patients with MV-CAD eligible for stent or surgery Exclude : Patients with acute STEMI, cardiogenic shock Randomized 1:1 MV-stenting With DES and ReoPro CABG With or without CPB All concomitant Meds shown to be beneficial are encouraged, including : Plavix, ACE inhibitors,b-blockers, statins etc PRIMARY: 5-year mortality SECONDARY: 12-month MACCE, 5-year Quality of Life FREEDOM
Integrilin plus STenting to Avoid myocardial Necrosis Trial PI: G. Sangiorgi, A. Colombo Co-PI: G. Biondi Zoccai
Eptifibatide double IV bolus Matched placebo ISTANT trial Coronary angiogram showing significant native coronary lesion treatable by means of >33 mm of DES Randomization Administration of 600 mg clopidogrel loading and heparin bolus in the catheterization laboratory In-hospital follow-up One-month follow-up Six-month follow-up
Take home messages • Gp IIb/IIIa inhibitors provided significant benefits in diabetics treated with PTCA or BMS • The introduction of high-dose clopidogrel loading has significantly improved peri-procedural outcomes, and likely limited the use of Gp IIb/IIIa inhibitors to selected cases (ie high-risk and/or ACS) • Their impact in diabetics undergoing PCI in the DES era has not yet been thoroughly established, but lack of evidence for an effect cannot be considered evidence for lack of an effect • Given the absence of specific data on diffuse disease, precise inference in this setting will have to wait for ongoing and future trials
For further slides on these topics please feel free to visit the metcardio.org website:http://www.metcardio.org/slides.html




![Diffuse Vascular Disease (Focus on Peripheral Arterial Disease [PAD])](https://cdn1.slideserve.com/3363465/slide1-dt.jpg)