Download
1 / 22
220 likes | 507 Views
Learning from the Recently Completed Oral Glycoprotein IIb/IIIa Receptor Antagonist Trials. Christopher Cannon, M.D. Brigham and Women’s Hospital Boston, MA. Need for Long-Term Antiplatelet Therapy. Markers of platelet activation persist at 1 month post ACS

E N D
Learning from the Recently Completed Oral Glycoprotein IIb/IIIa Receptor Antagonist Trials Christopher Cannon, M.D. Brigham and Women’s Hospital Boston, MA
Need for Long-Term Antiplatelet Therapy • Markers of platelet activation persist at 1 month post ACS • Ault K, et al. P selectin in the TIMI 12 trial. J Am Coll Cardiol 1999;33:634-639. • Events persist beyond acute period: In the TIMI 3 Registry, Death/MI/Rec Ischemia • In-hospital = 10.5% • One year = 28.3% • Benefit of IIb/IIIa inhibition achieved only during IV infusion period (PURSUIT, PRISM-PLUS)
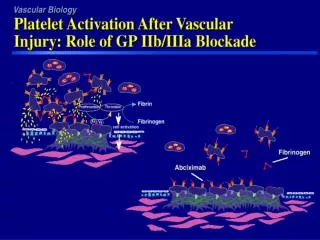
Activated Platelet GP IIb/IIIa 1. Platelet Adhesion Platelet GP Ib 2. Platelet Activation Plaque rupture ASA, Clopidogrel/Ticlopidine 3. Platelet Aggregation GP IIb/IIIa Inhibitors
CAPTURE 9.0% 4.8% 1,265 5.1% RESTORE 6.3% 2,139 EPILOG 9.1% 4.0% 2,792 PARAGON 11.7% 11.3% 2,282 PRISM 7.0% 5.7% 3,231 PRISM PLUS 11.9% 8.7% 1,570 GP IIb/IIIa Inhibitors in PCI and ACS Death/MI at 30 Days Trial Placebo IIb/IIIa Odds Ratio & 95% CI N EPIC 10.1% 7.0% 2,099 IMPACT-II 8.4% 7.1% 4,010 EPISTENT 10.2% 5.2% 2,399 PURSUIT 15.7% 14.2% 10,948 0.79 (0.73, 0.85) p < 10 -9 Overall 11.1% 9.0% 30,336 0 1 2 IIb/IIIa Better Placebo Better Topol EJ Lancet 1999;353:227-231.
TIMI-12: Oral IIb/IIIa Inhibition in ACS Major or Minor Bleeding Patients (%) mg bid mg qd n=52 11 69 59 72 5 9 47 Cannon et al. Circulation 1998;97:340
Study Design N= 10,302 Patient with Unstable Coronary Syndrome <72 hours ASA 150-162 mg daily Randomize 1:1:1 Orbofiban 50 mg BID Placebo BID Orbo 50 mg BID x 30 days then Orbo 30 mg BID Other Meds, Cath/Revasc per MD Primary endpoint to 30 days + follow-up Death, MI Urgent Revasc, Ischemia -> Rehosp, or Stroke F/U Day 14, Day 30 Follow-up visit every 3 months
Primary Endpoint - Through F/U (300 days) P values Each Dose vs. Placebo Orbo 50/30* 20.2 4.4 5.1 6.1 12.1 1.1 Orbo 50/50 20.1 4.1 5.4 6.1 11.2 1.1 No. Pts Composite (%) Death MI Urg revasc Rehosp Stroke Placebo 20.3 3.1 5.5 8.0 11.3 0.9 NS 0.002 / 0.03 NS 0.001 / 0.003 NS NS *Orbofiban 50mg bid x 30 days, then 30mg bid Data as of Jun 10 1999
Placebo Orbo 50/30 Orbo 50/50 No. Deaths reviewed Progressive Sudden Non-Ischemic Bleeding New Thrombotic Event 35 7 11 7 2 8 69 19 15 5 5 25 43 9 9 1 3 21 Cause of Deaths within 30 Days (Preliminary Review) Data as of Jun 10 1999
Bleeding Events and Thrombocytopenia (F/U) P value Each Dose vs. Placebo Orbo 50/30 1.2 0.2 2.2 3.3 0.6 0.3 0.3 Orbo 50/50 0.7 0.1 3.1 3.7 0.6 0.3 0.3 No. Pts Severe ICH Major Major/Sev Platelets 50-80,000 20-50,000 <20,000 Placebo 0.4 0.1 1.7 1.9 0.1 0.1 0.0 0.0001 / 0.04 NS NS / 0.0002 < 0.0001 0.0003 0.01 / 0.02 0.01/0.01 Data as of Jun 10 1999
CAPRIE Safety (Mean 2 year F/U) Clopidogrel Aspirin* (n = 9599) (n = 9586) • GI hemorrhage 2.0% 2.7% P < 0.05 • Hospitalizationdue to GI hemorrhage 0.7% 1.1% P = 0.012 • GI ulcers 0.7% 1.2% P < 0.001 • Intracranial hemorrhage 0.4% 0.5% P = NS • Severe Neutropenia 0.04% 0.02% P = NS • *Patients with a history of GI bleed and peptic ulcers were excluded from CAPRIE.
Primary Endpoint to F/UPatients-> PCI on study drug 30 % Patients 25 20 15 F/U pl v. 50-30: p=0.14 pl v. 50-50: p=0.02 10 5 placebo 30d pl v. 50-30: p=0.73 50-30 mg pl v. 50-50: p=0.08 50-50 mg 0 0 50 100 150 200 250 300 Data as of Jun 10 1999 Time (days)
Summary • First large global trial in ACS of oral IIb/IIIa inhibitor • Orbofiban: minimal efficacy benefit with small excess in mortality • Major bleeding and thrombocytopenia rates were low but higher than placebo • Greater benefit and no harm was seen in subgroups with normal renal function and without heart failure. • 30% benefit in PCI patients on study drug
The EXCITE Trial Randomization Placebo Placebo TID 6 Month Follow-up Xemilofiban 10 mg TID PTCR Xemilofiban 20 mg Xemilofiban 20 mg TID Stented patients were assigned to receive either ticlopidine (if assigned to the placebo arm) or ticlopidine placebo (if assigned to an active therapy arm ) for 2 to 4 weeks. ASA was taken by all patients at doses between 80-325 mg per day 30 to 90 min prior to PTCR
0.20 Treatment Placebo Xemilofiban 10 mg Xemilofiban 20 mg 0.15 Cumulative Event Rate 0.10 0.05 0 0 1 2 3 4 5 6 7 Month from Randomization Primary Efficacy Analysis(Death, MI, and Urgent Revascularization)
TIMI 12 / Symphony I Trials Sibrafiban 6 weeks 3 months D/MI/RI Death/MI
100 80 50 0 0h 6h 0h 6h IV vs. Oral GP IIb/IIIa inhibition Intravenous Oral 100 75 50 % inhibition (ADP) IV infusion: (Eptifibatide 180 ug/kg + 2.0 ug/kg/min) (mean +/- Std. Dev) N=48 25 Oral : (Orbofiban 50 mg BID) = Mean 0 0 6h 12h 24h 36h Data on File, COR/Key Ferguson et al JACC 1998;31:185A (abstract)
P-selectin Expression (percentage of platelets) ADP-Inducted Activation of Platelets from Patients Treated with Orbofiban Fibrinogen Binding Platelet Degranulation/P Selectin 0.2 µM ADP 2.0 µM ADP 100 100 p < 0.05 p < 0.01 80 80 (percentage of platelets) Fibrinogen Binding _ 60 60 _ _ 40 40 _ 20 20 0 0 Randomization 1 Month Randomization 1 Month Holmes et al. Am J Cardiol (in press)
Fibrinogen Binding and Platelet Aggregation with IIb/IIIa Inhibitor Fibrinogen Binding Platelet Aggregation P=0.001 Peter et al, Blood 1998;92:3230-9.
IIb/IIIa inhibitor Hypothesis: Intrinsic Activating Property of IIb/IIIa Inhibition GP IIb/IIIa Receptor FGN Unactivated Activated Activation of IIb/IIIa receptor Dissociation of competitive inhibitor Binding IIb/IIIa inhibitor FGN “Outside-In Signaling Platelet Activation Allows Binding of Fibrinogen + Plt Aggreg Platelet Adapted: Peter et al., Blood 1998;92:3230-9.
Exploratory Analyses: Lessons Learned Fixed-dosing with a competitive oral IIb/IIIa inhibitor: • Peaks/troughs in % inhibition and high inter-patient variability • Low blood levels at some time periods • Too low to prevent events • ? Proaggregatory effects (Peter et al, Blood 1998) • High blood levels in some patients ( creat.) • Potential for excess bleeding • ? Plaque hemorrhage -> increased events
Scorecard - Comparing Oral Agents 2nd Generation 1st Generation Oral IIb/IIIa inhibitors RoxifibanOrbofibanSibrafiban Xemilofiban TrialRocket OPUS-TIMI16 Symphony EXCITE IIb/IIIa selective +++ +++ +++ +++ Binding TightlyCompetitive Competitive Competitive bound “Off rate” 7 mins seconds seconds seconds Peak of Onset 3-6h 4-6h 4-6h 2-3h Half-life 24 h 8-10h 11h 4-5h Excretion Plt. Dissoc. Renal Renal Renal Dosing QD BID BID TID Low Peak/trough +++ ++ ++ + Intra-pt variability + ++ ++ ++ Inter-pt variability ++ ++ ++ ++ Plts < 50,000 <0.5% 0.6% <0.5% 0.5% Plts Pro-aggreg. No Yes - Yes
Conclusions - Oral Antiplatelet Therapy at the End of the Millennium • Future Directions - Oral IIb/IIIa inhibitors: 1. Need to optimize dosing • Mimic stable effect of IV drugs • Reduce inter- and intra-patient variability • ? Use bedside platelet test to adjust dose 2. Test “second generation” drugs (tight IIb/IIIa binding) • ASA and ADP antagonists • Proven benefit in large trials • Both decrease platelet activation • Combination ASA/Clopidogrel being tested