Download
1 / 38
440 likes | 1.21k Views
Vitamin D. metabolism. Presented by Deena Abdel Hadi Attended by Dr. A. B. Hamam. Introduction. Vitamin D. is a group of sterols having similar physiologic activity. Forms: D2-calciferol is activated ergosterol (plant origin).

E N D
Vitamin D. metabolism Presented by Deena Abdel Hadi Attended by Dr. A. B. Hamam.
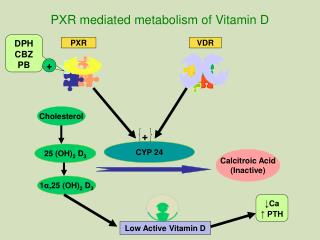
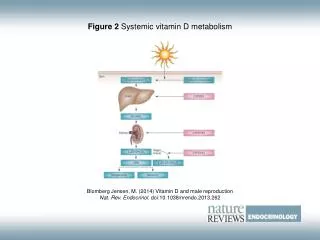
Introduction • Vitamin D. is a group of sterols having similar physiologic activity. • Forms: D2-calciferol is activated ergosterol (plant origin). D3 is activated 7-dehydrochelesterol in skin (animal origin). • Vitamin D3 is naturally present in human skin, the provitamin (7-dehydrocholesterol ) is activated photo chemically to vitamin D3 which is then transferred to the liver. Both vitamin D2 & D3 are hydroxylated (activated) in the liver to 25-OH-cholecalciferol &, subsequently, in the renal cortex to 1,25-dihydroxycholecalciferol, which functions as a hormone. Receptors for 1,25-dihydroxycholecalciferol are present in most tissues, but its 1ry roles are facilitation of : - Intestinal absorption of Ca & PO4. - Renal reabsorption of PO4. - A direct effect on bone deposition & reabsorption of Ca & PO4. - with parathormone & calcitonin, 1,25-dihydroxycholecalciferol plays a major role in Ca &PO4 homeostasis of both body fluids & body tissues.
Characteristics • Fat soluble. • Stable to heat, acid, alkali & oxidation. • Bile necessary for absorption.
Biochemical Action • Regulates absorption & deposition of Ca & PO4 by affecting permeability of intestinal membrane. • Regulates level of serum alkaline phosphatase, which is believed to be concerned with calcium phosphate deposition in bones & teeth.
Effects of Deficiency • Rickets. • Infantile Tetany. • Poor Growth. • Osteomalacia.
Rickets • Rickets is a general disorder of metabolism affecting chiefly the growing bones due to deficiency of vitamin D • Skeletal muscles & sometimes the nervous system are also affected . • The essential changes in bones are: 1) Decalcification of the normal bones already present. 2) Formation of imperfectly calcified new bone resulting in widening & enlargement of the epiphyseal end of the bone .
Etiology of Rickets • Deficiency of vitamin D(infantile Rickets). • Defective absorption of vitamin D & calcium(malabsorption syndromes). • Hepatic diseases(biliary atresia). • Use of anticonvulsants as the combination of phenobarbitone & phenytoin(these drugs accelerate degradation of vitamin D by the liver).
Etiology of Rickets • Renal diseases: 1) Defective 1-Alfa-hydroxylase enzyme (vitamin D dependant rickets type 1 ). 2) Glomerular ( renal osteodystrophy in CRF) 3) Tubular: - Renal tubular acidosis - Fanconi syndrome • End organ unresponsiveness (vitamin D dependant rickets type 2 ).
Vitamin D. Deficiency Rickets • Etiology: The deficiency of vitamin D usually results from prolonged breast feeding without Vit. D supplement & inadequate exposure to sun rays. • Factors help in pathogenesis of infantile Rickets: 1) Rapidity of bone growth in infancy. 2) Race(dark skin interferes with sunlight) 3) Season(more in winter).
4) Diet: • Vitamin D is present in diet such as liver, kidney, meat, egg yolk & cod liver oil. • CHO are poor in Vit. D, Ca & P. • Some diets are rachitogenic : - Ca/P ratio in breast milk is 2:1. This is the optimum ratio for absorption of Ca & P, in animal milks, the ratio is 1:1 resulting in reduction of absorption. - Cereals (high phytic acid, which hinders the absorption of Ca).
Pathology of Rickets The following 4 zones are encountered in the epiphyseal metaphyseal region of normal bones: • Zone of resting cartilage(which is formed of 1 layer of cells). • Zone of proliferating cartilage(which is formed of regular 6 layers). • Zone of provisional calcification [epiphyseal line](the cartilage cells in this layer become mature. They contain alkaline phosphatase which releases phosphates into the matrix that already contain Ca & phosphates in solution. The added phosphate ions will increase the product of Ca X PO4. Once the product exceeds 40, precipitation of calcium phosphate occurs in the matrix around these cells. This results in death of the cartilage cells as they are deprived from their nutritional supply). • Zone of bone formation(the layer of provisional calcification is invaded by blood capillaries &osteoblasts. The osteoblasts deposit a layer of organic bone matrix (ostoid tissue) which become rapidly mineralized. The calcified cartilage is ultimately replaced by bone).
Changes in infantile Rickets Vitamin D deficiency will lead to diminished Ca & PO4 absorption from the intestine.This will cause low Ca level in the blood hyperparathyroidism mobilization of Ca & PO4 from bones & decreases tubular reabsorption of phosphates in the kidney normal serum Ca & low serum PO4. Decreased CA available for bones Ca X PO4 will be far below 40 failure of calcification of the intercellular substance around the mature cartilage cells in the zone of provisional calcification as well as the ostoid tissue around the osteoblasts. THIS WILL PRODUCE THE FOLLOWING:
The mature cartilage cells will not die. The proliferating zone will be formed of many layers, it invades the adjacent zone of provisional calcification & hence the irregularity of the epiphyseal line in the X-ray. • The zone of provisional calcification fails to mineralize & newly formed osteoid tissue is not calcified or calcified irregularly. As a result a wide irregular frayed zone of non rigid tissue (the rachitic metaphysis) is produced. This layer is responsible for many of the skeletal deformities of rickets because it doesn’t have the rigidity of the normal bone cartilage junction & so it is liable to compression producing flaring of the ends of the bone & the rachitic rosary. • In the shaft, the performed bone is resorbed but it is also replaced by uncalcified osteoid tissue from the periosteum, which forms a shell surrounding the shaft over its entire length. The result is a soft rarified cortical bone, hence the bone deformities & green stick fractures.
Clinical Manifestations • After several months of vitamin D. deficiency, skeletal changes of rickets can be recognized. Breast fed infants whose mothers have osteomalacia may have rickets by 2 months of age. Florid rickets becomes apparent towards the end of the first & during the second year of life. In later childhood, rickets is rare. • Symptoms: Early (between 3-6 months) - head sweating. - irritability by day & sleeplessness by night. Advanced rickets: - delayed motor development (sitting, standing & walking).
Signs: 1) Bony Changes: Changes in the skeleton are greatest @ the sites where growth is most rapid & the deformities are the result of gravity & traction of muscles on the affected bones. A. Head: 1)Craniotabes:is the earliest bony changes to be observed. Its greater incidence is from 3-6 months of age. It usually disappears before the end of the first year. other causes of Craniotabes include: - Prematurity. - Osteogenesis imperfecta. - Hydrocephalus. The rachitic Craniotabes is present in localized areas away from the sutures, while in other causes it is present near the suture lines or is generalized.
2) Anterior fontanel: is wider & its closure is delayed than normal. 3) Frontal and parietal bossing:are due to deposits of osteoid tissue which are situated mainly around the centers of ossification of these bones. 4) Head size: looks larger than normal. 5) Head shape:the vault & occiput are flattened [this together with frontal & parietal bossings & the grooves between the bosses result in caput quadratum (the skull is square)]. 6)Teeth eruption: is usually delayed & deciduous teeth may show enamel defect or decay.
B. Thorax: 1) Rachitic rosary: beading of ribs @ costochondral junctions is another early sign & is seen as a row of nodules about the size of cherries extending down & backwards along the line of costochondral junctions. 2) Harrison sulcus: is a horizontal groove corresponding to the line of attachment of the diaphragm with flaring of the costal margin below. 3) Longitudinal grooves: due to yielding of the chest wall @ its weakest point which is the costochondral junction giving the picture of pigeon chest deformity. The groove is located just behind the rachitic rosary & is produced by compression of the ribs @ their weakest points by the atmospheric pressure. The sternum with its adjacent cartilages appear to be projected forwards.
C. Extremities: 1) Epiphyseal enlargement: is common & best felt @ the wrists & ankles. 2) Marfan’s sign: is a transverse groove that is felt over the malleoli just proximal to the ankle join. It is due to the excess osteoid tissue deposited in the centers of ossification of the lower ends of tibia & fibula &the malleoli. 3) Deformities: tibia & fibula often become curved after the rachitic child has started to walk resulting in bow legs or knock knees. The femur & tibia may show an anterior convexity. The humerus & the bones of the forearms may show convexity on their extensor surfaces as the infant crawls. 4) Fractures: of the green stick variety are often seen.
D. Pelvis: The pelvis in rickets is small & continue to be retarded in growth. The pelvis inlet is narrowed by a forward projection of the promontory of the sacrum & the outlet is narrowed by a forward projection of the tip of the coccyx . In females, these changes , if they become permanent , add to the hazards of the childbirth & may necessitates C/S.
2) Muscle & Ligaments: Hypotonia of the muscles & laxity of the ligaments are usually present, they lead to the following: 1. Delayed motor milestones as sitting & walking. 2. Flaccidity of the whole body which may lead to hyper extensibility of the joints. 3. Smooth kyphosis in the dorsolumbar region while sitting. It is correctable if the infant is suspended from the shoulder. Lordosis of the lumbar region may be seen in the erect position. Scoliosis may occur. 4. The abdomen is distended due to: - Hypotonia of the abdominal muscles & the muscles of the intestines. - Downward displacement of the liver & spleen due to Hypotonia of abdominal muscles, laxity of their ligaments & the deformity of the chest wall.
Complication of Rickets • Tetany: (the most important complication. It is usually precipitated by infections). • Recurrent chest infections due to: 1) Chest wall deformity. 2) If there is associated vitamin A deficiency (vitamin A is essential for the integrity of epithelial surfaces including respiratory mucosa). 3) Defective function of the immune system may occur (especially T lymphocytes). • Bone fractures. • Bone deformities.
Biochemical Changes in Rickets • Serum Ca is normal (2ry to compensatory hyperparathyroidism). • Serum PO4 is decreased (2ry to compensatory hyperparathyroidism). • Alkaline phosphatase in blood is increased. • Decreased 1,25-dihydroxy vitamin D in the serum.
Radiological Findings in Rickets • Active Rickets: X-ray of the wrists is best for early diagnosis, sine a characteristic changes of radius & ulna occur @ an early stage. The X-ray shows the following: 1) Broading + cupping (concave) +frying (irregular) of the lower ends of radius & ulna. This is the classic triad of rickets. 2) Increased distance between the distal ends of radius & ulna & the metacarpal bones. 3) Demineralization of the shafts. 4) Fractures & deformities may be present. 5) Periosteal elevation
Healing Rickets: The appearance of the line of preparatory calcification indicates start of healing. This line appears as faint narrow irregular band @ the region of metaphysis. As healing progresses the osteoid tissue between this line & the end of bone becomes calcified until they become united. Evidence of healing will appear in the X-ray between the 2nd & 3rd weeks.
Prevention Of Rickets • Exposure to U.V. rays. • A daily oral dose of 400 IU of vitamin D in the form of cod liver oil or one of the concentrates in water miscible form. The daily prophylactic dose of vitamin D recommended for prematures & twins is 1000 units. • Vitamin D should be given to the pregnant & lactating mother.
Treatment of Infantile Rickets • A daily administration of 1000-4000 units will produce healing in 2-4 weeks demonstrable in x-ray. Healing is complete in 6-8 weeks. • An alternative method of treatment is the oral or IM administration of one massive dose of vitamin D 600,000 IU that shouldn’t be repeated except if there is no evidence of healing by X-ray after one month. • Prevention & treatment of rickets (in severe rickets, it is better to keep the child off his feet until healing is well advanced. In cases of severe deformity, osteotomy is needed after complete healing of the rachitic process. • In prematures, in addition to vitamin D give also Ca (equivalent to 60 mg elemental Ca/day) & PO4 ( equivalent to 30 mg elemental P/day).
Infantile Tetany • Tetany is hyperirritability of the nervous system due to lack of active Ca ions. • Ca in the blood is present in 2 forms : - Active ionized Ca. - Non-ionized protein bound Ca [when the protein bound Ca decreases (e.g. in hypoproteinemia), hypocalcaemia will be present but without Tetany].
Etiology 1) Infantile Tetany(the commonest type) usually occurs as a complication of infantile rickets. It is usually precipitated by infections due to failure of parathyroid compensatory mechanism. 2) Hypoparathyroidism: occurs in Tetany of newborn. 3) Infants fed on cow’s milkmay get hyperphosphatemia & subsequent hypocalcaemic Tetany. 4) Excessive vomitingleading to alkalosis with resulting decrease in the ionized Ca. 5) Excess administration of alkalie.g. bicarbonate. 6) Hyperventilationleading o alkalosis e.g. in acute encephalitis. 7) Hypomagnesaemia.
Clinical Picture I. Manifest Tetany: It occurs when the level of serum Ca < 7mg/dl. Manifest Tetany may present by: 1) Carpo-pedal spasm: - In carpal (hand) spasm the interphalangeal joints extend, the metacarpophalangeal joints flex & the thumb is adducted across the palm & wrists flex. - In pedal (foot) spasm, the feet are inverted & toes are flexed. 2) Laryngeal spasm: where you get whooping sound especially on crying, its maximal occurrence is between 6-15 months. 3) Generalized convulsions.
II. Latent Tetany: Occurs when serum Ca is between 7-9mg/dl. The nerves are hyperirritable & ischemia, mechanical or electrical stimulation will lead to characteristic responses: A) Chovostek’s sign: tapping lightly with a patellar hummer in the region of exit of the facial nerve from the skull, about 3-5cm below & in front of the ear. The facial muscles twitch briefly with each tap. B) Trousseau’s sign: inflation of the sphygmomanometer cuff on the upper arm to more than the systolic blood pressure is followed by carpal spasm within four minutes. C) Peroneal sign: tapping the Peroneal nerve on the neck of fibula, the muscles it supplies contract leading to eversion of the foot. D) Erb’s sign: applying current less than 5 milliamperes, the stimulated muscle contract. Normally, a more powerful current is needed.
Diagnosis • Classic clinical picture of Carpo-pedal spasm + etiological condition as rickets. • Laboratory investigations: - Serum total Ca is below 7mg/dl. - Investigation for the cause as x-ray both wrists for evidence of rickets. • Cases of convulsions & laryngeal spasm must be thoroughly investigated before diagnosing Tetany as an etiology.
Management • I.V. Ca gluconate 10% (1-2cc/kg) is given immediately very slowly (to avoid cardiac arrest in systole). • I.V. diazepam 0.3mg/kg/dose may be needed in cases with generalized convulsions before Ca could be given. • Oral Ca gluconate or lactate 200-500mg/kg/day. • Treat any associated condition e.g. acute infections. • Investigate the etiological factor & treat the underlying cause e.g. administration of vitamin D if the patient is rachitic.
Effects of Excess • Wide variation in tolerance, over 500ug/day toxic when continued for weeks, prolonged administration of 45ug/day may be toxic. • Nausea. • Diarrhea. • Weight loss. • Polyuria. • Nocturia. • Soft tissue calcification (heart, renal tubules, blood vessels, bronchi & stomach).
Hypervitaminosis D. Clinical manifestation: • The patient feels weak, thirsty, anorexic & loses weight. • Nausea & vomiting. • Polydepsia & Polyuria. • Constipation. • Dehydration. • Kidneys (stone formation or nephrocalcinosis which may lead to renal failure. • Deposition of Ca in soft tissues around the joints & in the walls of blood vessels. Metastatic calcification may occur in the heart, lungs, thyroid & pancreas.
Laboratory findings: • Serum Ca increases. • Serum phosphorus is normal. It increases in renal failure. • Urinary Ca increases. Radiological findings: • Increased density of bones @ the growing ends. • Dense metaphyseal lines. • Ca deposition in soft tissues. • U/S scan for renal stones or nephrocalcinosis.
Treatment: • Stop administration of vitamin D. • Correct dehydration. • Decrease calcium in diet by stopping milk & its products or by increasing cereals in the diet to decrease calcium absorption . • Prednisone 2mg/kg/day is an effective antidote, it should be given until the serum Ca has fallen to 12mg/dl, then it should be stopped.
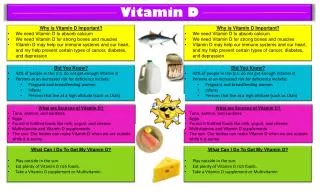
Sources • Vitamin D-fortified milk & margarine. • Liver. • Kidney. • Meat. • Egg yolk. • Fish liver oils. • Exposure to sunlight or other U.V. sources.
THE END Thank You