Download
1 / 44
440 likes | 879 Views
THERMOREGULATION. Peri-operative Teaching June 2008 Dr Mohua Jain Specialist Anaesthetist. Definitions. CORE TEMPERATURE PERIPHERAL TEMPERATURE NORMOTHERMIA HYPOTHERMIA. CORE TEMPERATURE Thermal compartment of body, highly perfused tissues, uniform and higher temperature.

E N D
THERMOREGULATION Peri-operative Teaching June 2008 Dr Mohua Jain Specialist Anaesthetist
Definitions • CORE TEMPERATURE • PERIPHERAL TEMPERATURE • NORMOTHERMIA • HYPOTHERMIA
CORE TEMPERATURE Thermal compartment of body, highly perfused tissues, uniform and higher temperature. Trunk, brain – 2/3 body heat • PERIPHERAL TEMPERATURE Skin, subcutaneous – all body, inc limbs Usually 2 to 3 °C below core but can be much more
Core and peripheral temperatures both influence comfort about equally. • Only core influences metabolic processes • As peripheral temp drops, heat flows from core to periphery (gradient)
NORMOTHERMIA Core temp range of 36°C to 38°C • HYPOTHERMIA Core temp less than 36°C • MILD HYPOTHERMIA Core temp range 34°C to 36°C
Definitions (NICE) • Preoperative - 1 hour before induction • Intraoperative - the total anaesthesia time • Postoperative - 24 hours after entry into the recovery area in the theatre suite • Hypothermia - a patient core temperature of below 36.0°C. • Comfortably warm - the expected normal temperature range of adult patients • Temperature - used to denote core temperature
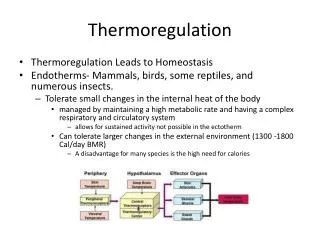
Maintenance of Heat • Balance of heat production and loss • Nervous system • Hormones • Vessels • Behaviour • Variations during day and month
Heat Production • Metabolism • Exercise • Shivering • Non-shivering thermogenesis (fat and muscle) • Basal metabolic rate (BMR) is energy needed to maintain constant temperature
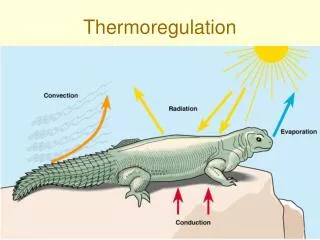
Heat Loss • Radiation (40 to 60%) • Convection (25 to 30%) • Evaporation (10 to 20%) • Respiration (10% by heating of air and evaporation) Energy loss can be up to 15 x BMR Sweating can be up to 1 litre per hour for short time, taking heat with it!
Don’t forget Hypothermia can be present regardless of temperature if patient complains of feeling cold or has the obvious signs Body needs to maintain set temperature as all processes involving enzymes are sensitive to temp and pH
Signs Usually below 36.5°C • Peripheral vasoconstriction (esp stressed patients) • Hairs standing on end (pilo-erection) • Shivering • Cold peripheries • High diastolic blood pressure Importance of ‘behavioural’ actions
Measurement of Core Temperature • accurate (patient, operator, instrument - variable readings) • consistent, • repeatable, • keeping up with rapid changes, • accessible, • safe
Core Temperature Measurement Sites RELIABLE ESTIMATE Rectal Bladder Oral Skin Axillary • Pulmonary artery • Tympanic membrane (direct and indirect) • Nasopharynx • Distal oesophagus
Adverse Effects of Hypothermia • CNS (Nervous system) • RS (Respiratory system) • CVS (Cardiovascular system) • Renal and electrolytes • Immune • Blood • Drug effects • Others
CNS • Reduced neuronal function • Confusion • Disorientation • Stupor • Raised intracranial pressure from shivering • Seizures • Coma
RS • Hyperventilation then hypoventilation • Lower respiratory rate • Lower volumes (effect on CNS) • Increased oxygen consumption from shivering • Organ ischaemia
CVS • More adrenaline (and other catecholamines) • Vasoconstriction • Raised blood pressure • Bradycardia • Myocardial ischaemia and infarction • ECG changes • Arrhythmias
Renal & Electrolytes ‘Cold diuresis’ • Renal tubule damage • Constriction of skin and gut vessels • Potassium, Magnesium, Calcium and Phosphate all decrease
Immune Infections Wound breakdown and infections • Collagen linking less as oxygen drops • Less subcutaneous oxygen • White blood cells function less
Blood • Less coagulation • Less platelet function • More viscosity • More blood loss • More blood transfusions
Drug effects • Usually prolongs actions of all drugs, (esp those needing enzymes for their metabolism) • Muscle relaxants and opiates last longer • Less IV and volatile agents needed for same degree of unconsciousness
Other • More patient discomfort with shivering • More time in PACU / Recovery • Thresholds for pain and nausea • Difficulty with cannulation • More time in hospital • More time to establish diet • More costs from all above
Shivering • Usually temperature related – uncomfortable involuntary rhythmic muscle contractions to maintain core temperature • Complex , patterns of tremors • Can occur post GA or during labour even with normal temperature. Mechanism unknown ?pain and stress • Post-op 20 to 40%? • Problem for monitoring • Elderly rarely shiver
Drugs to treat Post-op Shivering (clinical and experimental) • Tramadol • Pethidine • Alfentanil • MgSo4 • Clonidine • Ketamine • Propofol • Ondansetron • Doxapram • Nefopam • Meperidine • Ketanserin • Physostigmine
Effects of General and Regional Anaesthesia • Impaired thresholds for responses so they happen later • 3 stage drop in temperature 1 to 3°C • Rapid in 1st hour (Redistribution of heat from core to periphery - vasodilation) • Gradual (Heat loss causes then exceed heat production causes) • Plateau (Production catches up)
So far... • Definitions • Heat balance – how and why needed • Measurement of core temperature • Bad effects of Hypothermia • Shivering (normally and post-op) • Anaesthesia So, how can we prevent hypothermia?
Evidence - Research and Clinical • Recommendations and guidelines (esp 2000 onwards) • WHO - ambient temperature • American Society of Anesthesiologists (ASA) • American Society of PeriAnesthesia Nurses (ASPAN) • National Institute of Clinical Excellence (NICE)
Common Sense Guidelines • Minimising heat loss from the body • Giving heat to the body
Common Sense Guidelines • Pre-operative • Intra-operative • Post-operative • ASSESSMENT (identify, measure, observe & ask) • INTERVENTION (preventative, passive and active)
Identification of Risks • Very young • Very old • Female • GA / RA • Large surface area / gut exposed • Ambient temp (circulating air) • Poor nutritional status • Length of surgery • Fluid shifts • Irrigation fluids • Trauma/burns • Cold transfers
Patients at higher risk of perioperative hypothermia (NICE) Some patients are at higher risk of inadvertent perioperative hypothermia; they should be managed accordingly if any two of the following apply: • ASA grade II to V • preoperative temperature below 36.0°C • undergoing combined general and regional anaesthesia • undergoing major or intermediate surgery • at risk of cardiovascular complications.
Expectations • Core temperature never to drop below 36°C at any stage • To avoid symptoms and signs • If GA will last 30 mins or more, must measure temp through operation • More strict if high risk group • Start actions BEFORE theatre
Preoperative warming If the patient’s temperature is below 36.0°C in the hour before they leave the ward or emergency department: • forced air warming should be started preoperatively on the ward or in the emergency department (unless there is a need to expedite surgery because of clinical urgency) • forced air warming should be maintained throughout the intraoperative phase.
Intraoperative phase The patient’s temperature should be measured and documented before induction of anaesthesia and then every 30 minutes until the end of surgery. Induction of anaesthesia should not begin unless the patient’s temperature is 36.0°C or above.
Passive – to minimise heat loss For hypothermic AND normothermic patients • Ambient temp at least 20°C (upto 30° if burns or neonates!) • Passive insulation (layer of air) • Warmed cotton aircell blankets • Space blanket? • Circulating water mattress? • Hats (esp Paeds) Socks etc • (Special cases – pre veins, post flaps) • (Before – preop vasodilation)
Active – add to heat gain For hypothermic patients • Skin – Forced air warming / convective (Bair Hugger) – upto 50 W heat given (no infection evidence) • Internal – IV, irrigation (1 litre fluid at room temp will lower core temp by 0.25°C) • Airway - humidification (HMEF)
Cardiopulmonary bypass • Dialysis • (Protein infusion to increase metabolism) • Watch out for over-heating of skin and fluids (keep below 45°C)
Warming intravenous fluids Intravenous fluids (500 ml or more) and blood products should be warmed to 37°C using a fluid warming device.
Postoperative phase The patient’s temperature should be measured and documented on admission to the recovery room and then every 15 minutes • Ward transfer should not be arranged unless the patient’s temperature is 36.0°C or above. • If the patient’s temperature is below 36.0°C, they should be actively warmed using forced air warming until they are discharged from the recovery room or until they are comfortably warm
Discussion Which key areas of local practice differ from the guideline? To ensure effective implementation: what equipment is needed? what are staff training needs? What will the impact be on the average length of patient stay if the guideline is implemented fully? How should Risk and Safety Managers be involved in the implementation of the guideline?
SUMMARY • Understanding of heat balance • Understanding why this is important • Why to prevent temp below 36°C • How to measure temperature • Recommendations of how to assess • Passive and active ways of helping the patient from pre- to post-op