Download
1 / 52
520 likes | 576 Views
Explore the functions and effects of insulin in the body, from regulating glucose and fat metabolism to protein synthesis. Learn about diabetes mellitus and antidiabetic types of insulin preparations.

E N D
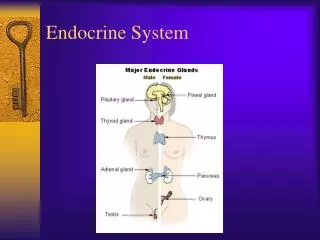
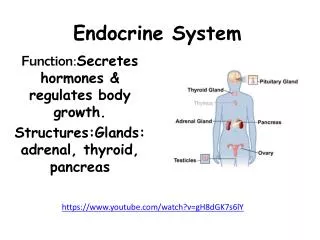
ENDOCRINE SYSTEM( 2) PRESENTED BY: ATTIYA MALIK CLINICAL PHARMACIST
ENDOGENOUS INSULIN Insulin is a protein hormone which is secreted by B cells the average adult pancrease secrete 40-60units of insulin daily. This include a basal amount of 1-2units /hr and additional amount of 4-6 units/hr after meals or when the blood sugar exceeds 100mg/dl.
Insulin secretion • Portal circulation. • Systemic circulation. After degradation it is transported to different body cells.in 10-15mints it is cleared from the blood .
Functions of insulin • Transport glucose to different compartments i.e. liver heart smooth muscle organs ,fats, muscle both fat and muscle is used to produce energy.
Effects of insulin • Carbohydrate metabolism. • Fat metabolism. • Protein metabolism.
Carbohydrate • Insulin regulates glucose metabolism to produce energy for cellular functions ,if excess glucose is present after this need Is met it is converted to glycogen and store for future energy needs or converted to fats and stored. The excess glucose is transported to liver cells is converted to fat only after glycogen stores are saturated.
Absent insulin • When insulin is absent or blood glucose levels are low these store from of glucose can be reconverted .the liver is especially very important in restoring blood sugar levels by breaking down glycogen or by forming new glucose.
FAT METABOLISM • Insulin promotes transport of glucose into the fat cells ,where it is broken down.one of the breakdown products is alpha glyceropohosphate which combines with fatty acids to form triglycerides .
Absent insulin • When insulin is lacking ,fat is release into the blood stream as free fatty acids. Blood concen of triglycerides ,cholesterol and phospholipids are also increase. The high levels increase the % age of atherosclerosis.
PROTEIN METABOLISM • Insulin increase the total amount of body protein by increasing transport of amino acids into the cells and synthesis of protein with in the cells. The basic mechanism of these effects is unknown. The loss of protein is are not compensated by new protein and protein wasting is an abnormality and cause severe weakness
DIABETES MELLITUS • The incident of diabetes is growing rapidly in the USA and world wide 135 million people are afflicted with the most common form TYPE 2 TYPE 1 . • Rather it is a heterogeneous group of syndromes characterized by elevation of blood glucose caused by relative or absolute deficiency of INSULIN
TYPE 2 DIABETES MELLIUTS • Rather than autoimmune response or viruses this disease is influenced by genetic factors obesity, aging peripheral insulin resistance . • In this blood glucose is not taken up of cells leads to hyperglycemia
SYMPTOMS • POLYDISPESIA. • POLYURIA. • DEHYDRATION. • POLYPHAGIA. • GLUCOURIA.
1: GLUCOURIA: a glucose level is increase 2 folds than the normal values and after wards kidney receive more glucose and that will entered into the renal tubules lead to more glucose into the urine. 2 :POLYURIA: Increase levels of glucose in blood lead to pull of water into the renal tubules which will cause more urine or loss of water . 3:POLYDEPSIA: When polyuria taken place it will lead to polydipsia a normal term for it is thirsty.
4: POLYPHAGIA: an increase of appetite is called polyphagia in which the diabetic is unable to digest the food and lead to weight loss.
TYPES OF INSULIN PREPARATIONS 1. Ultra-short-acting 2. Short-acting (Regular) 3. Intermediate-acting 4. Long-acting
3. Intermediate - acting insulins e.g. isophane (NPH Humulin N) Turbid suspension Injected S.C.(Only) Onset of action 1 - 2 hr Peak serum level 5 - 7 hr Duration of action 13 - 18 hr Insulin mixtures 75/25 70/30 50/50 ( NPH / Regular )
3. Intermediate - acting insulins (contd.) Lente insulin Turbid suspension Mixture of 30% semilente insulin 70% ultralente insulin Injected S.C. (only) Onset of action 1 - 3 hr Peak serum level 4 - 8 hr Duration of action 13 - 20 hr
3. Intermediate - acting insulins (contd.) Lente and NPH insulins Are roughly equivalent in biological effects. They are usually given once or twice a day. N.B: They are not used during emergencies (e.g. diabetic ketoacidosis).
4. Long – acting insulins e.g.Insulin glargine Onset of action 2 hr Absorbed less rapidly than NPH&Lente insulins. Duration of action upto 24 hr Designed to overcome the deficiencies of intermediate acting insulins Advantages over intermediate-acting insulins: Constant circulating insulin over 24hr with no pronounced peak. More safe than NPH&Lente insulins due to reduced risk of hypoglycemia(esp.nocturnal hypoglycemia). Clear solution that does not require resuspention before administration.
Methods of Adminisration • Insulin Syringes • Pre-filled insulin pens • External insulin pump Under Clinical Trials • Oral tablets • Inhaled aerosol • Intranasal, Transdermal • Insulin Jet injectors • Ultrasound pulses
COMPLICATIONS OF INSULIN THERAPY 1. Severe Hypoglycemia (< 50 mg/dl )– Life threatening Overdose of insulin Excessive (unusual) physical exercise A meal is missed How it is treated ? 2. Weight gain 3. Local or systemic allergic reactions (rare) 4. Lipodystrophy at injection sites 5. Insulin resistance 6. Hypokalemia
Oral Hypoglycemics All taken orally in the form of tablets. Pts with type11 diabetes have two physiological defects: • Abnormal insulin secretion • Resistance to insulin action in target tissues associated with decreased number of insulin receptors
Oral Anti-Diabetic Agents Drugs other than Sulfonylurea Sulfonylureas
Sulfonylureas (Oral Hypoglycemic drugs) First generation Second generation Long acting Short acting Long acting Short acting Intermediate acting Glyburide (Glibenclamide) Glimepiride Chlorpropamide Glipizide Tolbutamide Acetohexamide Tolazamide
MECHANISM OF ACTION OF SULPHONYLUREAS 1) Release of insulin from β-cells 2) Reduction of serum glucagon concentration 3) Potentiation of insulin action on target tissues
SIDE EFFECTS OF SULPHONYLUREAS 1) Nausea, vomiting, abdominal pain, diarrhea 2) Hypoglycaemia 3) Dilutional hyponatraemia & water intoxication (Chlorpropamide) 4) Disulfiram-like reaction with alcohol (Chlorpropamide) 5) Weight gain
CONTRAINDICATIONS OF SULPHONYLUREAS 1) Type 1 DM ( insulin dependent) 2) Parenchymal disease of the liver or kidney 3) Pregnancy, lactation 4) Major stress
Drugs other than Sulfonylurea Meglitinides Biguanides α-Glucosidase Inhibitors Thiazolidinediones Repaglinide Nateglinide Metformin Rosiglitazone Pioglitazone Acarbose
MEGLITINIDES e.g. Repaglinide, Nateglinide PHARMACOKINETICS Taken orally Rapidly absorbed ( Peak approx. 1hr ) Metabolized by liver t1/2 = 1 hr Duration of action 4-5 hr
MEGLITINIDES (Contd.) MECHANISM OF ACTION Bind to the same KATP Channel as do Sulfonylureas, to cause insulin release from β-cells.
MEGLITINIDES (Contd.) CLINICAL USE Approved as monotherapy and in combination with metformin in type 2 diabetes Taken before each meal, 3 times / day Does not offer any advantage over sulfonylureas; Advantage: Pts. allergic to sulfur or sulfonylurea SIDE EFFECTS: Hypoglycemia Wt gain ( less than SUs ) Caution in pts with renal & hepatic impairement.
BIGUANIDES e.g. Metformin PHARMACOKINETICS Given orally Not bind to plasma proteins Not metabolized Excreted unchanged in urine t 1/2 2 hr
BIGUANIDES (Contd.) MECHANISM OF ACTION 1. Increase peripheral glucose utilization 2. Inhibits gluconeogenesis 3. Impaired absorption of glucose from the gut
Advantages of Metformin over SUs Does not cause hypoglycemia ( why ? ) Does not result in wt gain ( why ? ) ( Ideal for obese pts )
BIGUANIDES (Contd.) SIDE EFFECTS 1. Metallic taste in the mouth 2. Gastrointestinal (anorexia, nausea, vomiting, diarrhea, abdominal discomfort) 3. Vitamin B 12 deficiency (prolonged use) 4. Lactic acidosis ( rare – 01/ 30,000-exclusive in renal & hepatic failure)
THIAZOLIDINEDIONE DERIVATIVES New class of oral antidiabetics e.g.: Rosiglitazone Pioglitazone
THIAZOLIDINEDIONE DERIVATIVES (Contd.) PHARMACOKINETICS • 99% absorbed • Metabolized by liver • 99% of drug binds to plasma proteins • Half-life 3 – 4 h • Eliminated via the urine 64% and feces 23%
THIAZOLIDINEDIONE DERIVATIVES (Contd.) MECHANISM OF ACTION • Increase target tissue sensitivity to insulin by: • reducing hepatic glucose output & increase glucose uptake & oxidation in muscles & adipose tissues. • They do not cause hypoglycemia (similar to metformin and acarbose ) .
THIAZOLIDINEDIONE DERIVATIVES (Contd.) ADVERSE EFFECTS • Mild to moderate edema • Wt gain • Headache • Myalgia • Hepatotoxicity ?
THIAZOLIDINEDIONE DERIVATIVES (Contd.) INDICATIONS Type 11 diabetes alone or in combination with metformin or sulfonylurea or insulin in patients resistant to insulin treatment.
GOALS OF THERAPY • Maintain blood glucose levels or near normal levels. • Promote normal metabolism of carbohydrates, fats,protein, and acute and long term complications. • Prevent hypoglycemic episodes. • To avoid micro and macro complications.