Download
1 / 1
10 likes | 201 Views
Management of Polytrauma in Explosive-Blast Injury T. Wong, A. Matsou , A. Hancox, K. Miller, P. Mahoney, T. Torlinski University Hospitals Birmingham NHS Foundation Trust, Royal Centre for Defensive Medicine. Scene Day 0: 0 Hours

E N D
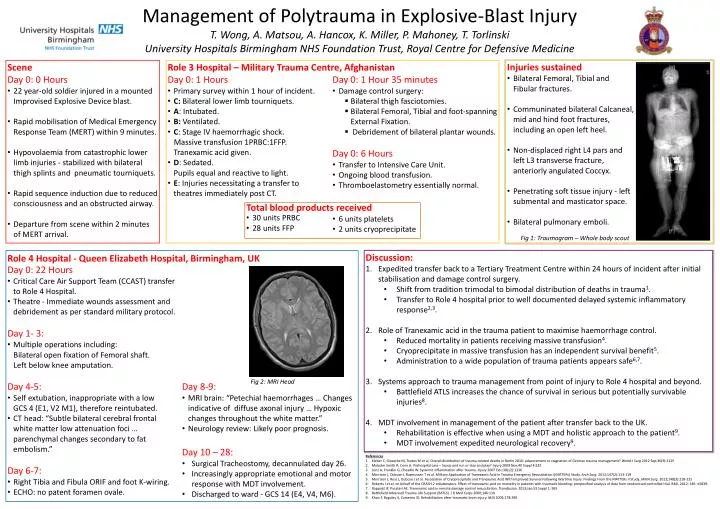
Management of Polytrauma in Explosive-Blast InjuryT. Wong, A. Matsou, A. Hancox, K. Miller, P. Mahoney, T. TorlinskiUniversity Hospitals Birmingham NHS Foundation Trust, Royal Centre for Defensive Medicine • Scene • Day 0: 0 Hours • 22 year-old soldier injured in a mounted Improvised Explosive Device blast. • Rapid mobilisation of Medical Emergency Response Team (MERT) within 9 minutes. • Hypovolaemia from catastrophic lower limb injuries - stabilized with bilateral thigh splints and pneumatic tourniquets. • Rapid sequence induction due to reduced consciousness and an obstructed airway. • Departure from scene within 2 minutes of MERT arrival. • Injuries sustained • Bilateral Femoral, Tibial and Fibular fractures. • Communinated bilateral Calcaneal, mid and hind foot fractures, including an open left heel. • Non-displaced right L4 pars and left L3 transverse fracture, anteriorly angulated Coccyx. • Penetrating soft tissue injury - left submental and masticator space. • Bilateral pulmonary emboli. • Day 0: 1 Hours • Primary survey within 1 hour of incident. • C: Bilateral lower limb tourniquets. • A: Intubated. • B: Ventilated. • C: Stage IV haemorrhagic shock. • Massive transfusion 1PRBC:1FFP. • Tranexamic acid given. • D: Sedated. • Pupils equal and reactive to light. • E: Injuries necessitating a transfer to • theatres immediately post CT. • Day 0: 1 Hour 35 minutes • Damage control surgery: • Bilateral thigh fasciotomies. • Bilateral Femoral, Tibial and foot-spanning External Fixation. • Debridement of bilateral plantar wounds. • Day 0: 6 Hours • Transfer to Intensive Care Unit. • Ongoing blood transfusion. • Thromboelastometry essentially normal. Role 3 Hospital – Military Trauma Centre, Afghanistan Total blood products received • 30 units PRBC • 28 units FFP • 6 units platelets • 2 units cryoprecipitate Fig 1: Traumogram – Whole body scout • Day 0: 22 Hours • Critical Care Air Support Team (CCAST) transfer to Role 4 Hospital. • Theatre - Immediate wounds assessment and debridement as per standard military protocol. • Day 1- 3: • Multiple operations including: • Bilateral open fixation of Femoral shaft. • Left below knee amputation. • Day 4-5: • Self extubation, inappropriate with a low • GCS 4 (E1, V2 M1), therefore reintubated. • CT head: “Subtle bilateral cerebral frontal • white matter low attenuation foci … parenchymal changes secondary to fat embolism.” • Day 6-7: • Right Tibia and Fibula ORIF and foot K-wiring. • ECHO: no patent foramen ovale. • Day 8-9: • MRI brain: “Petechial haemorrhages … Changes indicative of diffuse axonal injury … Hypoxic changes throughout the white matter.” • Neurology review: Likely poor prognosis. • Day 10 – 28: • Surgical Tracheostomy, decannulated day 26. • Increasingly appropriate emotional and motor response with MDT involvement. • Discharged to ward - GCS 14 (E4, V4, M6). • Discussion: • Expedited transfer back to a Tertiary Treatment Centre within 24 hours of incident after initial stabilisation and damage control surgery. • Shift from tradition trimodal to bimodal distribution of deaths in trauma1. • Transfer to Role 4 hospital prior to well documented delayed systemic inflammatory response2,3. • Role of Tranexamic acid in the trauma patient to maximise haemorrhage control. • Reduced mortality in patients receiving massive transfusion4. • Cryoprecipitate in massive transfusion has an independent survival benefit5. • Administration to a wide population of trauma patients appears safe6,7. • Systems approach to trauma management from point of injury to Role 4 hospital and beyond. • Battlefield ATLS increases the chance of survival in serious but potentially survivable injuries8. • MDT involvement in management of the patient after transfer back to the UK. • Rehabilitation is effective when using a MDT and holistic approach to the patient9. • MDT involvement expedited neurological recovery9. Role 4 Hospital - Queen Elizabeth Hospital, Birmingham, UK Fig 2: MRI Head References Kleber C, GieseckeM, Tsokos M et al. Overall distribution of trauma-related deaths in Berlin 2010: advancement or stagnation of German trauma management? World J Surg 2012 Sep;36(9):2125 Malcolm Smith R, Conn A. Prehospital care – Scoop and run or stay and play? Injury 2009 Nov;40 Suppl 4:S23 Lenz A, Franklin G, Cheadle W. Systemic inflammation after trauma. Injury 2007 Dec;38(12):1336 Morrison J, Dubose J, Rasmussen T et al. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Arch Surg. 2012;147(2):113-119 Morrison J, Ross J, Dubose J et al. Association of Cryoprecipitate and Tranexamic Acid With Improved Survival Following Wartime Injury. Findings From the MATTERs II Study. JAMA Surg. 2013;148(3):218-225 Roberts I et al; on behalf of the CRASH-2 collaborators. Effect of tranexamic acid on mortality in patients with traumatic bleeding: prespecified analysis of data from randomised controlled trial. BMJ. 2012; 345: e5839. RappoldJF, Pusateri AE. Tranexamic acid in remote damage control resuscitation. Transfusion. 2013;Jan;53 Suppl 1: 96S Battlefield Advanced Trauma Life Support (BATLS). J R Med Corps 2000;146:110 Khan F, Baguley IJ, Cameron ID. Rehabilitation afeer traumatic brain injury. MJA 2003;178:290