Download
1 / 21
210 likes | 345 Views
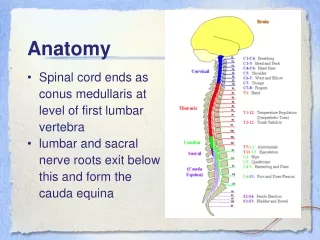
It’s SOOO tiny--in comparison to the adult airway. A little swelling or mucous goes a long way!. The alveoli, surfactant properties and alveolar capillaries are not well-developed until after week 30 of gestation. Anatomy. What makes the pediatric airway so fragile?. Child Anatomy

E N D
It’s SOOO tiny--in comparison to the adult airway. A little swelling or mucous goes a long way! The alveoli, surfactant properties and alveolar capillaries are not well-developed until after week 30 of gestation... Anatomy What makes the pediatric airway so fragile?
Child Anatomy 1. Proportionally larger head 2. Smaller Nostrils 3. Larger Tongue 4. Decreased Muscle Tone 5. Longer and more horizontal epiglottis 6. More anterior larynx 7. Cricoid=Narrowest portion 8. Shorter Trachea 9. Narrower Airways ANATOMY
ANATOMY Slota, M. Core Curriculum for Pediatric Critical Care Nursing. 1998
Physical Inspection Palpation Percussion Auscultation History Prenatal and Delivery Childhood history Other Significant Info Chest pain Growth and development Gastrointestinal symptoms Sleeping habits Assessment: Key Points
Assessment • Inspection cont. • Respiratory effort • rate, rhythm, depth (excursion), effort • Quality of voice and breathing • muffled voice, wheezing, cough • Skin color and appearance • cyanosis, clubbing
Auscultation pitch, intensity, quality, duration of each breath compare side to side adventitious breath sounds crackles wheezing rhonci Abnormal Findings: Stridor inspiratory expiratory both Cyanosis central or blue discoloration of skin Oxygen first! Cough many times age specific describe type Assessment: Key Points
RESPIRATORY RATES AgeRate Newborn 35-60 1-11 months 30-50 2 years 23-48 4 years 23-45 6 years 21-38 8 years 20-32 (1- 8 years ~20-40) 10 years 19-26 14 years 18-26 16 years 17-24 18 years 16-18 (> 8 years ~ < 20)
Respiratory Assessment • Mental Status • Color • Respiratory Rate • Work of Breathing • Air Movement
Normal Breath Sounds • Normal • Clear, soft inspiratory vesicular sounds • 1:2 ratio - Inspiration/Expiration • expiration is twice as long as inspiration
Constriction or Narrowing • Wheezing on inspiration or expiration • Whistling type noises produced during exhalation (sometimes inhalation) • Forced air through airways narrowed by bronchoconstriction, secretions, or mucosal edema • Causes are asthma, foreign body, COPD • If only on inspiration: it is stridor
Constriction or Narrowing • Stridor • Caused by upper airway being obstructed usually swelling or foreign body constriction • Inspiratory wheeze, high pitched “crowing” sound • Auscultate it high in the neck • Will be accompanied by muffled voice, difficulty swallowing, and at times drooling
Fluids or Secretions • Crackles • Scratchy inspiratory sounds • Most common sound in small children • Sound made by alveoli opening with fluid or secretions in or around them • Usually in lower lobes first • Causes • Atelectasis (collapsed or under inflated alveoli) • Pneumonia (consolidation of fluid/inflammation)
Fluids or Secretions • Rhonchi • Gurgling type sound (like the last bits of a milk-shake through a straw) • Sound made by secretions that form or collect in the large airways • Can sometimes be cleared with suctioning or coughing • Causes • Bronchitis • Aspiration
Adventitious Sounds • Decreased or Diminished Sounds • Pulmonary congestion causes sound transmission to the chest edges. • No or low air movement results in few sounds • Causes • Pneumonia • Pleural effusions • Asthma
Adventitious Sounds • Grunting • Expiratory sound • Caused by the closing of the epiglottis at the end of expiration • Children with restrictive lung diseases grunt to increase residual capacity.
Identifying DistressBe able to recognize normal from abnormal!! • Normal • Abnormal • Serious • Crisis
Normal Exam • Mental Status - Awake and curious • Skin Color - Pink • Respiratory Rate - Normal for age • Work of Breathing - No extra work • Air Movement - Airflow full and regular
Abnormal Exam Mental Status - Restless Skin Color - Pale Respiratory Rate - Increased rate Work of Breathing – Dyspneic, diaphoretic Air Movement - Deep and rapid
Serious Abnormal Exam • Mental Status – Agitated, inattentive • Skin Color - Mottled and cool • Respiratory Rate - Irregular • Work of Breathing - Nasal flaring, retractions • Air Movement - Rapid and shallow
Crisis Exam • Mental Status - Depressed mental state • Skin Color - Cyanotic and cool • Respiratory Rate - Slow or absent • Work of Breathing - Accessory muscles, retractions • Air Movement - Shallow
DISTRESS Retractions Controlled Oxygen Requirement Tachypneic Mild grunting Secretions FAILURE Significant hypoxemia (high o2 requirement or PaO2 less than 60 mmHg) Hypercarbia (CO2 greater than 55 mmHg) Acidosis Altered Level of Consciousness Are You Worried? Distress vs. Failure