Download
1 / 58
600 likes | 659 Views
Learn about perinatal mortality, congenital malformations, causes, high-risk pregnancies, investigations, and management strategies to reduce perinatal deaths and birth defects.

E N D
Perinatal mortalityCongenital malformationsBirth traumaDr Renu Singh
Perinatal mortality(PNM) • Includes late fetal deaths &early neonatal deaths • Late fetal deaths (stillbirths): ≥ 28 weeks gestation till delivery • Early neonatal deaths: ≤ 7 days of birth • Perinatal mortality in developed nations :<10 per 1000 births • Developing countries: high,32-35 per 1000 in India
Definition • Perinatal mortality: all fetal & neonatal deaths weighing 1000g or more between 28 weeks of gestation to first week of neonatal life(WHO) • Perinatal mortality rate: expressed in terms of perinatal deaths per 1000 total births
Factors affecting PNM • Maternal age • Teenage pregnancies, elderly gravida • Parity • Anemia, inadequate prenatal care, inadequate rest, Malpresentation, multiple births • Socioeconomic factors • Lower socioeconomic status vs upper strata • Obstetric factors • Placental insufficiency, APH, intrapartum care, malpresentation ,multiple births
Causes of PNM • Antenatal causes • Maternal diseases, APH • Intranatal causes • Birth injuries, prolonged & difficult labor • Birth asphyxia • Postnatal causes • Prematurity • RDS • Respiratory, alimentary tract infections • Congenital malformations • Unknown: 30-35%
At risk pregnancies • Low socioeconomic status • Elderly gravida, • Teenage pregnancy • Poor past obstetric history • Malnutrition & severe anemia • Multiple pregnancy • Present pregnancy complications
Perinatal mortality rate • India (2010): 32 per 1000 births • Kerala: 12 per 1000 births • UP: 35 per 1000 births • Rajasthan: 37 per 1000 births • Odisha: 41 per 1000 births • MP: 42 per 1000 births
Reducing PNM • Education ,Improving living standards, raise social status • Universal prenatal care for all • Identify at risk pregnancies • Facilitate early & timely transfer of high risk women to higher centre • Strengthen the referral system • Essential newborn care to all,neonatal resuscitation • Accessible neonatal services
Congenital malformations • Structural abnormality which is present at birth • Incidence of fetal malformations: 2-5% • Account for 20% of perinatal deaths • WHO estimate: 2.76 million perinatal deaths due to congenital malformations(2013)
Terminology • Malformation: an abnormality of the development process (spina bifida) • Deformation: mechanical interference with normal development (talipes) • Disruption: interference with normal growth after a period of normal development(bowel atresia)
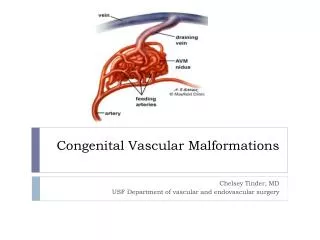
etiology • Chromosomal abnormalities: Trisomy (21,13,18),XO • Single gene mutation: Achondroplasia(AD) • Genetic predisposition • Multifactorial: NTD, congenital heart defects, cleft lip, palate • Drugs : lithium,valproate • Infection during pregnancy: Rubella,CMV • Mechanical factors: Talipes, potter sequence
High risk pregnancies • Uncontrolled diabetes in mother • Elderly gravida • Exposure to teratogenic drugs in 1st trimester • Maternal rubella in first trimester • H/O an affected sibling • Polyhydramnios/oligoamnios • Fetal growth restriction • Single umbilical artery
investigations • Biochemical screen: • MSAFP • Acetylcholine-esterase,hCG,uE3,inhibin A • Ultrasound soft markers • Echogenic foci in heart, echogenic bowel, pyelactasis • Ultrasonography • detailed structural anatomy,2D/3D • Targeted imaging for fetal anomalies(TIFA) • DM, hypothyroid, antiepileptic drugs
Investigations • Invasive procedures • CVS(chorionic villus sampling): obtain chorionic tissue • Amniocentesis: amniotic fluid • Cordocentesis: fetal blood • Fetoscopy : see fetal malformations • Fetal echocardiography: suspected CVS anomalies ,diabetes
Congenital malformations • Malformations of the CNS: • spina bifida, anencephaly, hydrocephalus • Skeletal malformations • Clubfoot, congenital dislocation of hip, skeletal dysplasias • GIT malformations • Omphalocele, gastroschisis, ilealatresia, duodenal atresia,Tracheoesophageal fistula • Genitourinary abnormalities • CVS abnormalities
Spina bifida • Failure of closure of the neural tube • Spina bifida occulta: defect is covered with skin • Spina bifida aperta: swelling seen over the spinal defect with defective skin covering • Meningocele • Myelomeningocele(spinal cord is involved) • Cephaloencephalocele(brain tissue involved)
Spina bifida • Lumbar defects : common • Complications associated are • Paralysis of lower limbs • Urinary ,fecal incontinence • Hydrocephalus • Limb deformity • Prognosis:60% survive with severe mental & physical handicap in 1/3rd ( immediate closure of defect)
anencephaly • Rudimentary brain with absent cerebral hemispheres ,absent vault • Most severe form of NTD • Prenatal diagnosis as early as 14 weeks • Offered MTP • Uniformly lethal
NTD: screening & prevention • MSAFP at 16-18 weeks : elevated ,2.5 MoM(95% DR) • Targeted Ultrasonography • Prognosis : Site &size of lesion, associated anomalies • Prevention: periconceptional administration of folic acid • Low risk women: 0.4-0.5 mg /day • h/o NTD: 5mg/day • Role of preconception counseling
Exomphalos • Midline abdominal wall defect • Herniation of bowel contents or liver into the umbilical stump with membranous covering • Raised MSAFP, USG,invasive prenatal procedures • Associated chromosomal abnormalities • Treatment is surgical
gastroschisis • Prolapse of intestine through paramedian abdominal wall defect • No covering membrane • Urgent surgical treatment
omphalocele Gastroschisis
Cleft lip ,cleft palate • Cleft lip(hare lip): unilateral/bilateral • Cleft palate: defect in roof of hard palate • Associated abnormalities: micrognathia /retrognathia • Feeding difficulties ,more with cleft palate • Small plastic plate ,obturator fits into the roof blocks the opening ,helps in feeding • Definitive t/t: surgery:3-4mths(hare lip),1-1/2 yrs
Birth trauma • Injuries sustained during labor & delivery • Stillbirth,neonatal deaths,morbidities • Important cause of PNM
Predisposing factors • Prolonged labor,obstructed labor • Fetal macrosomia • CPD • Malpresentation(breech) • Instrumental delivery(forceps/ventouse) • Shoulder dystocia • Precipitate labor • Internal podalic version
cephalhematoma • Blood collection between pericranium & flat skull bone • Unilateral, over parietal bone • Rupture of small emissary vein • Forceps delivery, normal delivery • Never present at birth, develops over 12-24 hrs • Swelling limited by suture lines • Good prognosis, blood gets absorbed in 6-8 wks • Vs.Caput succadaneum,meningocele
Intracranial hemorrhage • Traumatic • Fracture of skull bone : extradural or subdural hemorrhage • Neurological symptoms: acutely or insidious onset(vomiting, irritability) • Massive subdural hemorrhage : tear of tentorium cerebelli, injury to superior saggital sinus
Intracranial hemorrhage • Mechanism of tentorial tear • Excessive moulding in deflexed vertex with gross CPD • Rapid compression & decompression of after coming head of breech • Forcible forceps traction after wrong application of blades • Outcome: fatal, severe respiratory depression
Anoxic ICH • Intraventricular : intense congestion of fragile choroidal plexus due to anoxia • Subarachnoid: tear of tributary veins from brain to sinuses • Intracerebral: petechial hemorrhage in brain substance due to anoxia
Prevention of intracranial injuries • Comprehensive antenatal & intranatal care • Intensive fetal monitoring during labor : early detection of fetal hypoxia • Avoid difficult or traumatic vaginal delivery • Breech delivery: liberal use of CS,precautions while delivering limbs & aftercoming head • Vit.K 1mg IM after birth
Treatment of ICH • Supportive treatment • Maintain temperature,humidity,oxygen • Feeding by nasogastric tube,maintain fluid balance • Anticonvulsants: phenobarbitone(5-10mg/kg/day in divided doses) ,6 hrly intervals,IM • Subdural tap/surgical removal of clot
Skin & subcutaneous tissue • Bruises & lacerations over Face • Edematous & bruised scalp • Buttocks, genitalia gets edematous & bruised in breech presentation • Eyelids, nose,lips get bruised in face presentation • Needs no treatment
Muscles • Sternomastoid hematoma • Junction of upper & middle third • Appears 7-10 days after birth • Rupture of muscle fibres & blood vessels • Difficult breech delivery, excessive lateral flexion of neck in normal delivery, shoulder dystocia • Conservative, disappears by 6 mths age
Nerve injuries • Facial nerve palsy • Direct pressure of forceps blade • Hemorrhage & edema around nerve • Eye of affected side remains open • Angle of mouth drawn to unaffected side • Usually disappears in weeks, if isolated • Erb’s palsy • 5th & 6th cervical nerve roots involved • Waiter’s tip(extension of elbow, pronation of forearm, flexion of wrist)
Nerve injuries • Klumpke’s palsy • 7th ,8th cervical or 1st thoracic nerve roots • Arm flexed at elbow,forearm supinated ,claw like deformity of hand • Horner’s syndrome(homolateral ptosis,small pupil) • treatment • Splint • Full recovery, permanent disability
Fracture long bones • Fracture femur, humerus,radius,ulna • Breech delivery • Greenstick or complete type:X-ray • Rapid union occurs with callus formation • Deformity is rare • Treatment: splinting, closed reduction & casting
Prevention of newborn injuries • Screen out the high risk women in antenatal period: CPD, malpresentation::CS • Intranatal period • Continuous fetal monitoring • Difficult forceps to be avoided • Judicious selection of suitable candidates for instrumental delivery • Breech delivery by skilled personnel
Perinatal mortality • Role of fetal autopsy: ability to pick up minor anomalies /anomalies not detected on USG • Ethical, religious concerns • Careful examination, photograph & radiograph of fetus • Postmortem MR imaging : structural information of CNS anomalies • Helps in identifying the cause of fetal loss • Facilitates genetic counseling
Summary • Perinatal mortality is high in developing countries • India : 32per 1000 births(rural:35,urban:22) • Comprehensive antenatal and intranatal care is key to success in reduction of birth trauma & subsequently reduction in perinatal mortality • At birth ,essential newborn care to all
MCQ1 • Babies chosen for perinatal statistics include all except • Late fetal deaths • Early neonatal deaths • Body length (CHL) of 35 cm • 800 g at birth
MCQ1 • Babies chosen for perinatal statistics include all except • Late fetal deaths • Early neonatal deaths • Body length (CHL) of 35 cm • 800 g at birth
MCQ2 • One of the following drug is safe in pregnancy • Thalidomide • Sodium valproate • Ferrous sulfate • coumarins
MCQ2 • One of the following drug is safe in pregnancy • Thalidomide • Sodium valproate • Ferrous sulfate • coumarins