Download
1 / 22
240 likes | 501 Views
Prevention of Coronary Artery Disease PAS-880. Robert D. Hadley, PhD, PA-C July 19, 2001. What is CAD?. Coronary artery insufficiency and blockage, resulting in angina and MI CAD is one facet of systemic vascular disease

E N D
Prevention of Coronary Artery DiseasePAS-880 Robert D. Hadley, PhD, PA-C July 19, 2001
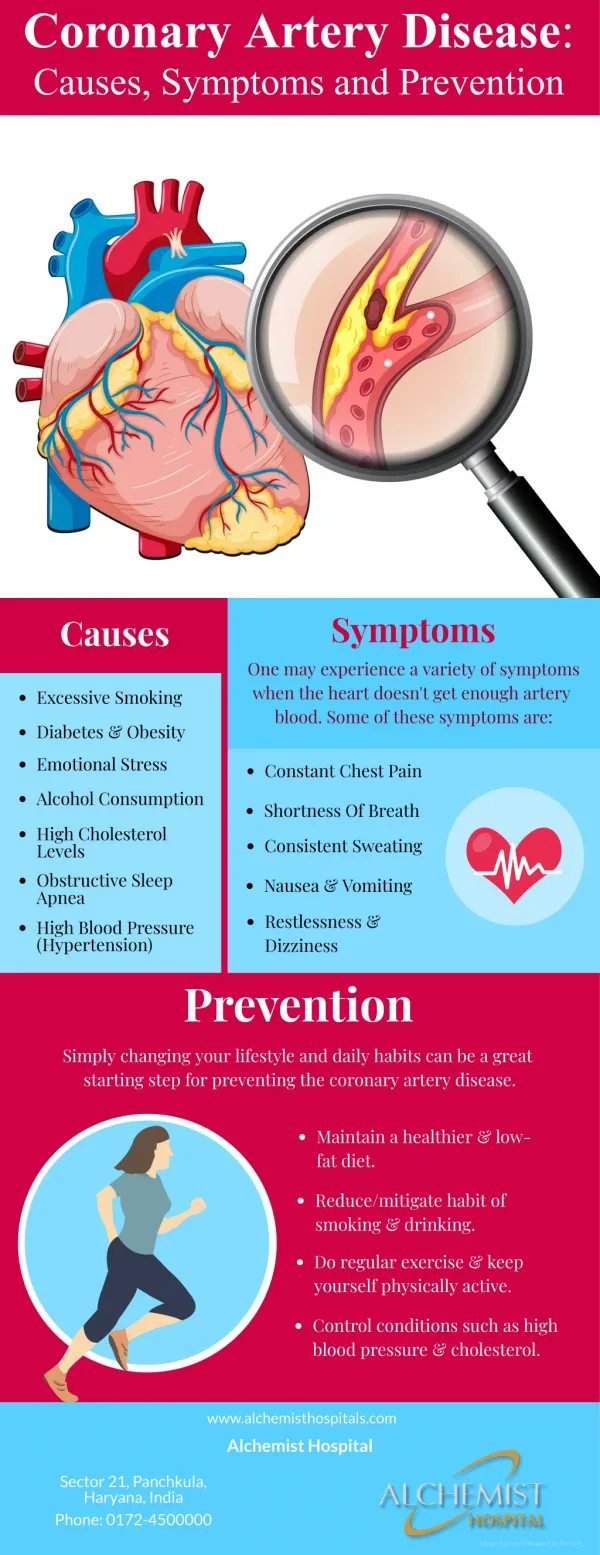
What is CAD? • Coronary artery insufficiency and blockage, resulting in angina and MI • CAD is one facet of systemic vascular disease • Vascular disease is largely due to inflammatory mechanisms in the vascular endothelium • Lesser contribution of “cholesterol buildup”
Vascular Endothelial Dysfunction • Related to multiple disease processes • Oxidative damage to endothelial cells • Much related to mechanical stress of HTN • Lipids • Accelerated atherosclerosis when combined with oxidative damage
Cardiovascular Dysmetabolic Syndrome “Syndrome X”: • Increased triglycerides, LDL, decreased HDL • Obesity (esp. central) • HTN • Diabetes/ glucose intolerance/ insulin resistance/ hyperinsulinemia • Increased PAI-1, inflammatory markers
PAI-1 • Plasminogen Activator Inhibitor • Plasmin comes from plasminogen, and dissolves clots • Plasminogen is activated by Plasminogen Activator • PAI-1 inhibits PA, resulting in hypercoaguability • PAI-1/PA should be in balance
Coronary Artery Disease • Unstable plaque, rather than gradual arterial narrowing is the problem in MI • Controlling factors that lead to plaque (especially unstable) will reduce risk of CAD
Risk Factors • Uncontrollable Risk Factors • Controllable Risk Factors
Heredity Gender Age Choose your parents well Choose your gender well Don’t age Uncontrollable Risk Factors
Controllable Risk Factors • Hypertension • Diabetes • Obesity • Hyperlipidemia • Smoking • Sedentary Lifestyle • Stress
Hypertension • Damage to vascular endothelium • AHA goals • 140/90 if no other risk factors • 135/85 (or lower) if other CV risk factors • Lifestyle changes– everyone! • Medicines • ACE-I/ ARB, b-blockers, diuretics
Diabetes • DCCT and UKPDS trials showed benefits of controlling sugar • Especially impt. to control HTN (Syndrome X) • UKPDS trial showed benefit of specific drugs in reducing CV risk • Combination therapy and exercise
Obesity • Epidemic, especially in US (Syndrome X) • Lose weight to “normal range”, with BMI of 18.5-24.9 (BMI= wt./height2, kg/m2) • J-shaped curve for overall mortality • Rate of 10% of body wt. over 6 mo, 1-2 lb/wk, avoid yo-yo effect • 1 lb = 3,500 Calories intake
Hyperlipidemia • Clear increased risk with elevated lipids • Goals depend on other risk factors, likely to be revised soon by NCEP • HDL>60, LDL<100/80, TG<200 for high risk person • Statins (HMG Co-A reductase inhibitors) probably have special status
Smoking • Don’t do it • Multiple substances contribute to inflammatory reaction in vascular endothelium • Cessation is extremely difficult • Nicotine itself is not the culprit, use nicotine replacements, keep trying • Nicotine more addictive than heroin
Sedentary Lifestyle • Exercise! • But how? • Moderate aerobic exercise better than strenous • Walking is usually best form of exercise • Accessible, no specialized equipment needed • Easily modulated, to maintain appropriate level of exertion • 30 min, 3 times a week, fast enough to slightly increase breathing rate
Stress • Contribution unclear, but has an effect on immune function and promotes inflammatory mediators • Exercise is best stress reducer • Other lifestyle modifications as necessary (divorce, etc.)
Alcohol? • What kind of EtOH? • Recent report* shows all-cause mortality benefit (much cardiovascular) of all kinds of EtOH, but wine a little better • 1-2 drinks/day for men, 1/2-1 /day for women • J-shaped curve *Ann. Int. Med. 133(6):411-419, 2000
Aspirin • Low dose aspirin of proven benefit • 81-325 mg qd or qod • Enteric coated • Few contraindications • Decreases clotting pathway and prevents thromboembolism
Hormone Replacement • Postmenopausal estrogen replacement previously thought to be strongly cardioprotective, with 25-50% reduction in risk of CVD • HERS study* and others** have questioned this effect • Other benefits still hold, but jury is still out on CVD *JAMA 280:605-613, 1998 **NEJM 343(8):522-529, 2000
Recent Report on HRT: • Low dose estrogen and estrogen/ progesterone (0.45 mg vs. usual 0.625 mg), some dose-related differences • 10% increase in HDL, 5% decrease in LDL after 1 yr of 0.45 mg estrogen • Improved thrombogenic markers (PAI-1, plasminogen) • Relatively young population (avg 51 yo) Fertility and Sterility 76(1): 13-24, July, 2001
Patient Education • Assess risk factors and inform Pt. • Smoking cessation, exercise, adherence to other disease management plans • If Pt. drinks, inform about the benefits of moderation • Inquire about and assess readiness to change, reassess at follow-up • If you give up, the patient surely will • If you don’t give up, the patient may change– eventually